

Learning curve and performance in simulated difficult airway for the novel C-MAC® video-stylet and C-MAC® Macintosh video laryngoscope: A prospective randomized manikin trial
- PMID: 33211728
- PMCID: PMC7676690
- DOI: 10.1371/journal.pone.0242154
Learning curve and performance in simulated difficult airway for the novel C-MAC® video-stylet and C-MAC® Macintosh video laryngoscope: A prospective randomized manikin trial
Abstract
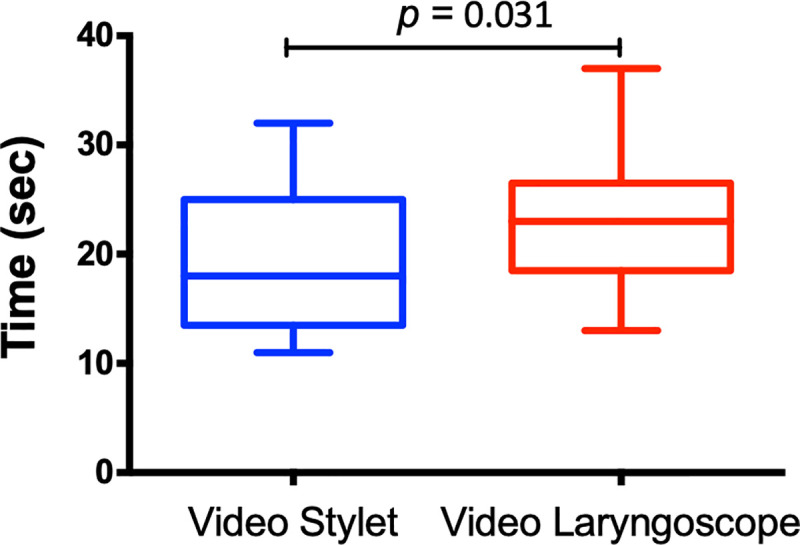
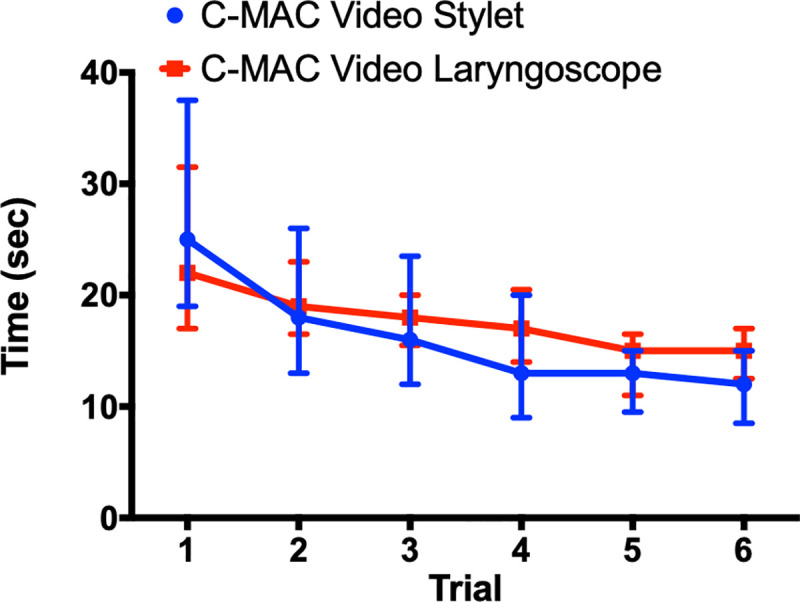
Difficult airways can be managed with a range of devices, with video laryngoscopes (VLs) being the most common. The C-MAC® Video-Stylet (VS; Karl-Storz Germany), a hybrid between a flexible and a rigid intubation endoscope, has been recently introduced. The aim of this study is to investigate the performance of the VS compared to a VL (C-MAC Macintosh blade, Karl-Storz Germany) with regards to the learning curve for each device and its ability to manage a simulated difficult airway manikin. This is a single-center, prospective, randomized, crossover study involving twenty-one anesthesia residents performing intubations on a Bill 1™ (VBM, Germany) airway manikin model. After a standardized introduction, six randomized attempts with VL and VS were performed on the manikin. This was followed by intubation in a simulated difficult airway (cervical collar and inflated tongue) with both devices in a randomized fashion. The primary end-point of this study was the total time to intubation. All continuous variables were expressed as the median [interquartile range] and analyzed using the Mann-Whitney U test. A 2-way ANOVA with Bonferroni's post hoc test was used to compare both devices at each trial. All reported p values are two sided. The median total time to intubation on a simulated difficult airway was faster with the VS compared to VL (17 [13.5-25] sec vs 23 [18.5-26.5] sec, respectively; 95% CI; P = 0.031). Additionally, on a normal airway manikin, the VS has a comparable learning curve to the VL. In this manikin-based study, the novel VS was comparable to the VL in terms of learning curve in a normal airway. In a simulated difficult airway, the total time to intubation, though likely not clinically relevant, was faster with the VS to the VL. However, given the above findings, this study justifies further human clinical trials with the VS to see if similar benefits-faster time to intubation and similar learning curve to VL-are replicated clinically.
Conflict of interest statement
JP declares that no competing interests exist. RRN: recipient of honoraria from Karl Storz, Germany for lectures at Euroanesthesia. Karl-Storz had no role in the present study and was not involved in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Figures
Comment in
-
The use of an epidural catheter for "spray-as-you-go" with the C-MAC video stylet.J Clin Anesth. 2023 Nov;90:111214. doi: 10.1016/j.jclinane.2023.111214. Epub 2023 Jul 23. J Clin Anesth. 2023. PMID: 37490797 No abstract available.
Similar articles
-
[Comparison of five video laryngoscopes and conventional direct laryngoscopy : Investigations on simple and simulated difficult airways on the intubation trainer].Anaesthesist. 2015 Jul;64(7):513-9. doi: 10.1007/s00101-015-0051-5. Epub 2015 Jul 15. Anaesthesist. 2015. PMID: 26174747 German.
-
Comparison of various video laryngoscopes for nasotracheal intubation in simulated difficult airway scenarios: a randomized self-controlled crossover trial.Expert Rev Med Devices. 2025 Jun;22(6):633-641. doi: 10.1080/17434440.2025.2499150. Epub 2025 May 4. Expert Rev Med Devices. 2025. PMID: 40289402 Clinical Trial.
-
Comparison of Macintosh and Intubrite laryngoscopes for intubation performed by novice physicians in a difficult airway scenario.Am J Emerg Med. 2017 May;35(5):796-797. doi: 10.1016/j.ajem.2017.01.005. Epub 2017 Jan 5. Am J Emerg Med. 2017. PMID: 28139309
-
Systematic Review and Meta-Analysis of Randomized Controlled Trials (RCTs) Revealing the Future of Airway Management: Video Laryngoscopy vs. Macintosh Laryngoscopy for Enhanced Clinical Outcomes.Cureus. 2023 Dec 17;15(12):e50648. doi: 10.7759/cureus.50648. eCollection 2023 Dec. Cureus. 2023. PMID: 38229823 Free PMC article. Review.
-
Video Versus Direct Laryngoscopy in Novice Intubators: A Systematic Review and Meta-Analysis.Cureus. 2022 Sep 25;14(9):e29578. doi: 10.7759/cureus.29578. eCollection 2022 Sep. Cureus. 2022. PMID: 36312614 Free PMC article. Review.
Cited by
-
Topical Anaesthesia Using a Soft Mist Spray Device Allows Comfortable Awake Visualisation of the Airway via Self-Videolaryngoscopy in Volunteers.Medicina (Kaunas). 2024 Jan 19;60(1):176. doi: 10.3390/medicina60010176. Medicina (Kaunas). 2024. PMID: 38276056 Free PMC article.
-
Simulation in airway management teaching and training.Indian J Anaesth. 2024 Jan;68(1):52-57. doi: 10.4103/ija.ija_1234_23. Epub 2024 Jan 18. Indian J Anaesth. 2024. PMID: 38406347 Free PMC article.
-
Successful intubation with a flexible optical stylet in a patient with predictors of difficult airway using pharyngeal clearance technique with a laryngoscope: A case report.Med Int (Lond). 2025 May 5;5(4):40. doi: 10.3892/mi.2025.239. eCollection 2025 Jul-Aug. Med Int (Lond). 2025. PMID: 40386188 Free PMC article.
-
Development of endotracheal intubation devices for patients with tumors.Am J Cancer Res. 2022 Jun 15;12(6):2433-2446. eCollection 2022. Am J Cancer Res. 2022. PMID: 35812038 Free PMC article. Review.
-
Simulation-based airway research: The fast-track recipes?Indian J Anaesth. 2022 Jun;66(6):395-398. doi: 10.4103/ija.ija_501_22. Epub 2022 Jun 21. Indian J Anaesth. 2022. PMID: 35903595 Free PMC article. No abstract available.
References
-
- Piepho T, Cavus E, Noppens R, Byhahn C, Dörges V, Zwissler B, et al. S1 guidelines on airway management. Der Anaesthesist. 2015;64(1):27–40. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
