

Differences in Opioid Overdose Mortality Rates Among Middle-Aged Adults by Race/Ethnicity and Sex, 1999-2018
- PMID: 33211981
- PMCID: PMC8093836
- DOI: 10.1177/0033354920968806
Differences in Opioid Overdose Mortality Rates Among Middle-Aged Adults by Race/Ethnicity and Sex, 1999-2018
Abstract
Objectives: The types of opioids abused in the United States have changed from prescription opioids to heroin to fentanyl. However, the types of opioids abused may differ by demographic factors, especially among middle-aged adults. We examined national trends in opioid overdose mortality rates among middle-aged adults by race/ethnicity and sex.
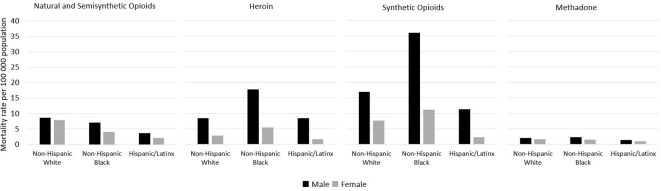
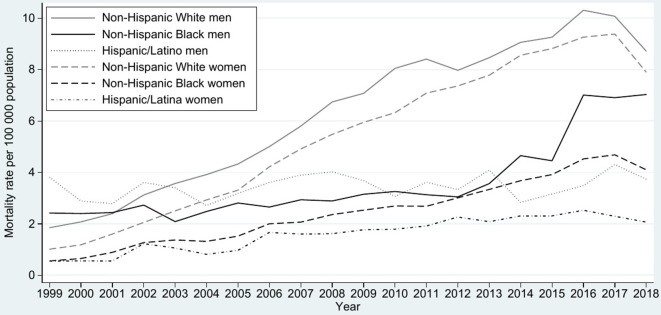
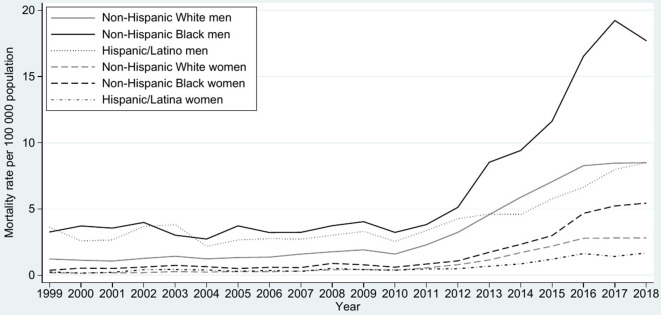
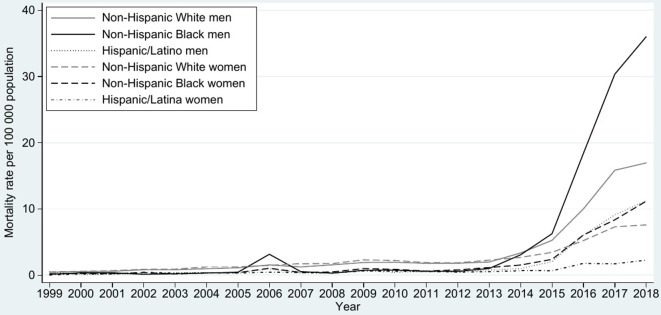
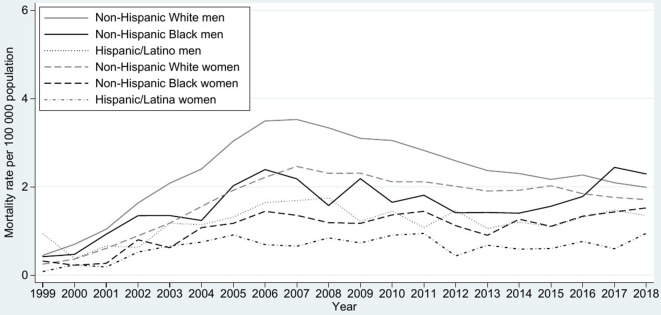
Methods: Using 1999-2018 data from the Centers for Disease Control and Prevention Wide-ranging ONline Data for Epidemiologic Research database, we examined overdose mortality rates per 100 000 population in 2018 among adults aged 45-64 that involved natural and semisynthetic opioids, heroin, synthetic opioids (excluding methadone), and methadone. We tested for significant differences in mortality rates by race/ethnicity and sex. We plotted drug-specific trends by race/ethnicity and sex from 1999 to 2018.
Results: In 2018, non-Hispanic White adults had the highest rates per 100 000 population of natural and semisynthetic overdose mortality (men: 8.7; women: 7.9; P < .001), and non-Hispanic Black adults had the highest rates of heroin (men: 17.7; women: 5.4; P < .001) and synthetic opioid (men: 36.0; women: 11.2; P < .001) overdose mortality. Men had significantly higher overdose mortality rates than women did for deaths involving natural and semisynthetic opioids, heroin, and synthetic opioids, but not methadone. From 1999 to 2018, mortality rates increased sharply for heroin and synthetic opioids, increased modestly for natural and semisynthetic opioids, and decreased for methadone. The greatest increases were among non-Hispanic Black men for heroin overdose (3.3 in 1999 to 17.7 in 2018) and synthetic opioid overdose (0.1 in 1999 to 36.0 in 2018).
Conclusions: Policy making should consider unique subgroup risks and alternative trajectories of opioid use other than people being prescribed opioids, developing opioid use disorder, subsequently moving to heroin, and then to fentanyl.
Keywords: Black or African American; Hispanic or Latino; White; mortality; opioid overdose.
Conflict of interest statement
Figures
References
-
- Manchikanti L., Kaye AM., Knezevic NN. et al. Responsible, safe, and effective prescription of opioids for chronic non-cancer pain: American Society of Interventional Pain Physicians (ASIPP) guidelines. Pain Physician. 2017;20(2 suppl):S3-S92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
