

Estimates of the global burden of cervical cancer associated with HIV
- PMID: 33212031
- PMCID: PMC7815633
- DOI: 10.1016/S2214-109X(20)30459-9
Estimates of the global burden of cervical cancer associated with HIV
Erratum in
-
Correction to Lancet Glob Health 2020; published online Nov 16. https://doi.org/10.1016/S2214-109X(20)30459-9.Lancet Glob Health. 2021 Feb;9(2):e119. doi: 10.1016/S2214-109X(20)30509-X. Epub 2020 Nov 20. Lancet Glob Health. 2021. PMID: 33227256 Free PMC article. No abstract available.
Abstract
Background: HIV enhances human papillomavirus (HPV)-induced carcinogenesis. However, the contribution of HIV to cervical cancer burden at a population level has not been quantified. We aimed to investigate cervical cancer risk among women living with HIV and to estimate the global cervical cancer burden associated with HIV.
Methods: We did a systematic literature search and meta-analysis of five databases (PubMed, Embase, Global Health [CABI.org], Web of Science, and Global Index Medicus) to identify studies analysing the association between HIV infection and cervical cancer. We estimated the pooled risk of cervical cancer among women living with HIV across four continents (Africa, Asia, Europe, and North America). The risk ratio (RR) was combined with country-specific UNAIDS estimates of HIV prevalence and GLOBOCAN 2018 estimates of cervical cancer to calculate the proportion of women living with HIV among women with cervical cancer and population attributable fractions and age-standardised incidence rates (ASIRs) of HIV-attributable cervical cancer.
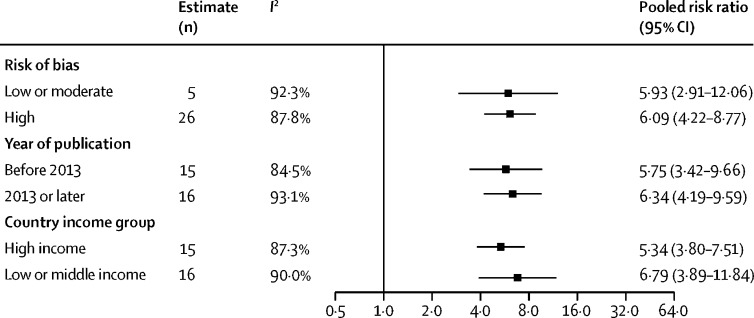
Findings: 24 studies met our inclusion criteria, which included 236 127 women living with HIV. The pooled risk of cervical cancer was increased in women living with HIV (RR 6·07, 95% CI 4·40-8·37). Globally, 5·8% (95% CI 4·6-7·3) of new cervical cancer cases in 2018 (33 000 new cases, 95% CI 26 000-42 000) were diagnosed in women living with HIV and 4·9% (95% CI 3·6-6·4) were attributable to HIV infection (28 000 new cases, 20 000-36 000). The most affected regions were southern Africa and eastern Africa. In southern Africa, 63·8% (95% CI 58·9-68·1) of women with cervical cancer (9200 new cases, 95% CI 8500-9800) were living with HIV, as were 27·4% (23·7-31·7) of women in eastern Africa (14 000 new cases, 12 000-17 000). ASIRs of HIV-attributable cervical cancer were more than 20 per 100 000 in six countries, all in southern Africa and eastern Africa.
Interpretation: Women living with HIV have a significantly increased risk of cervical cancer. HPV vaccination and cervical cancer screening for women living with HIV are especially important for countries in southern Africa and eastern Africa, where a substantial HIV-attributable cervical cancer burden has added to the existing cervical cancer burden.
Funding: WHO, US Agency for International Development, and US President's Emergency Plan for AIDS Relief.
© 2020 World Health Organization; licensee Elsevier. This is an Open Access article published under the CC BY 3.0 IGO license which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Figures



References
-
- Simms KT, Steinberg J, Caruana M. Impact of scaled up human papillomavirus vaccination and cervical screening and the potential for global elimination of cervical cancer in 181 countries, 2020–99: a modelling study. Lancet Oncol. 2019;20:394–407. - PubMed
-
- Vaccarella S, Laversanne M, Ferlay J, Bray F. Cervical cancer in Africa, Latin America and the Caribbean and Asia: regional inequalities and changing trends. Int J Cancer. 2017;141:1997–2001. - PubMed
-
- Arbyn M, Antoine J, Mägi M. Trends in cervical cancer incidence and mortality in the Baltic countries, Bulgaria and Romania. Int J Cancer. 2011;128:1899–1907. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
