

Age-Related Development of Cardiac Remodeling and Dysfunction in Young Black and White Adults: The Coronary Artery Risk Development in Young Adults Study
- PMID: 33212181
- PMCID: PMC8026546
- DOI: 10.1016/j.echo.2020.11.002
Age-Related Development of Cardiac Remodeling and Dysfunction in Young Black and White Adults: The Coronary Artery Risk Development in Young Adults Study
Abstract
Background: Little is known about the timing of preclinical heart failure (HF) development, particularly among blacks. The primary aims of this study were to delineate age-related left ventricular (LV) structure and function evolution in a biracial cohort and to test the hypothesis that young-adult LV parameters within normative ranges would be associated with incident stage B-defining LV abnormalities over 25 years, independent of cumulative risk factor burden.
Methods: Data from the Coronary Artery Risk Development in Young Adults study were analyzed. Participants (n = 2,833) had a mean baseline age of 30.1 years; 45% were black, and 56% were women. Generalized estimating equation logistic regression was used to estimate age-related probabilities of stage B LV abnormalities (remodeling, hypertrophy, or dysfunction) and logistic regression to examine risk factor-adjusted associations between baseline LV parameters and incident abnormalities. Cox regression was used to assess whether baseline LV parameters associated with incident stage B LV abnormalities were also associated with incident clinical (stage C/D) HF events over >25 years' follow-up.
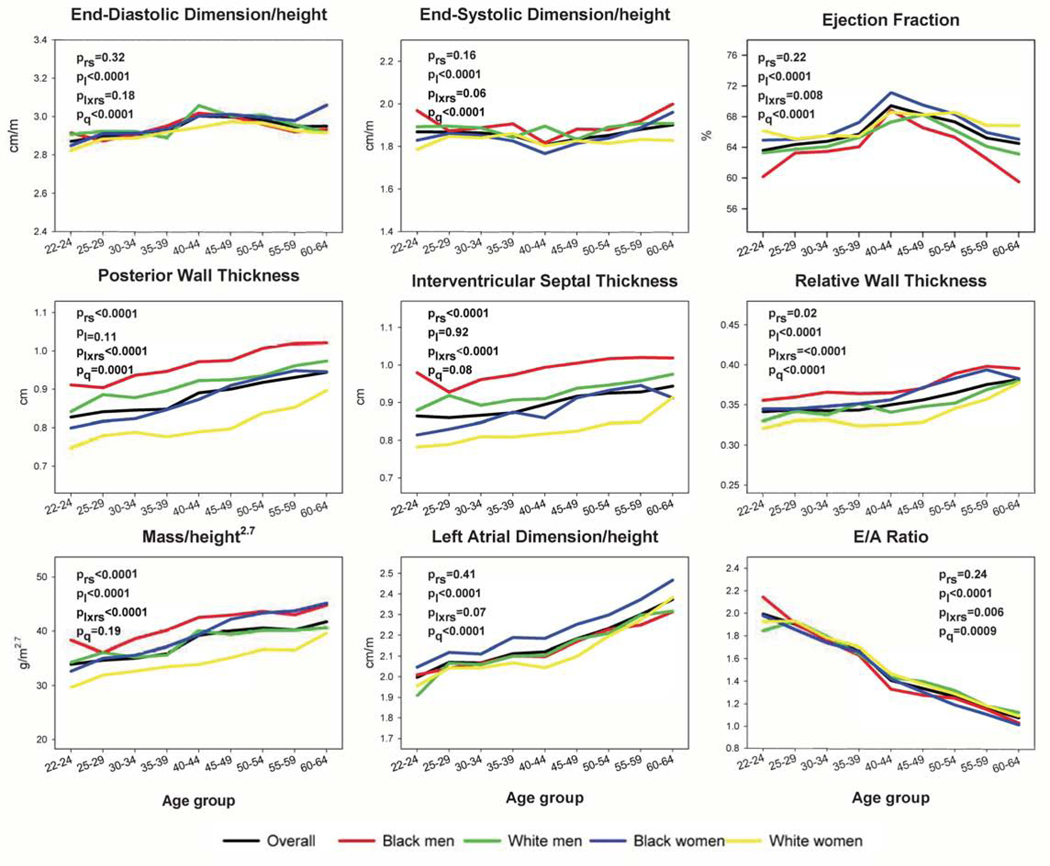
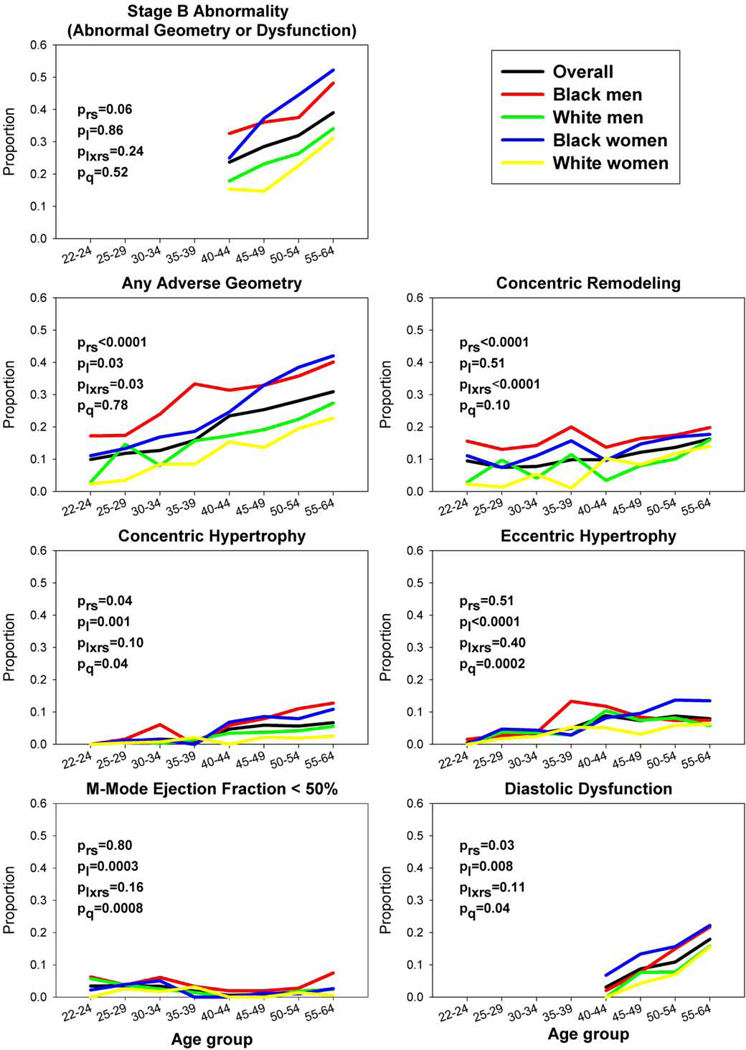
Results: Probabilities of stage B LV abnormalities at ages 25 and 60 years were 10.5% (95% CI, 9.4%-11.8%) and 45.0% (95% CI, 42.0%-48.1%), with significant race-sex disparities (e.g., at age 60, black men 52.7% [95% CI, 44.9%-60.3%], black women 59.4% [95% CI, 53.6%-65.0%], white men 39.1% [95% CI, 33.4%-45.0%], and white women 39.1% [95% CI, 33.9%-44.6%]). Over 25 years, baseline LV end-systolic dimension indexed to height was associated with incident systolic dysfunction (adjusted odds ratio per 1 SD higher, 2.56; 95% CI, 1.87-3.52), eccentric hypertrophy (1.34; 95% CI, 1.02-1.75), concentric hypertrophy (0.69; 95% CI, 0.51-0.91), and concentric remodeling (0.68; 95% CI, 0.58-0.79); baseline LV mass indexed to height2.7 was associated with incident eccentric hypertrophy (1.70; 95% CI, 1.25-2.32]), concentric hypertrophy (1.63; 95% CI, 1.19-2.24), and diastolic dysfunction (1.24; 95% CI, 1.01-1.52). Among the entire cohort with baseline echocardiographic data available (n = 4,097; 72 HF events), LV end-systolic dimension indexed to height and LV mass indexed to height2.7 were significantly associated with incident clinical HF (adjusted hazard ratios per 1 SD higher, 1.56 [95% CI, 1.26-1.93] and 1.42 [95% CI, 1.14-1.75], respectively).
Conclusions: Stage B LV abnormalities and related racial disparities were present in young adulthood, increased with age, and were associated with baseline variation in indexed LV end-systolic dimension and mass. Baseline indexed LV end-systolic dimension and mass were also associated with incident clinical HF. Efforts to prevent the LV abnormalities underlying clinical HF should start from a young age.
Keywords: Disparities; Heart failure; Left ventricle.
Copyright © 2020 American Society of Echocardiography. All rights reserved.
Figures
Comment in
-
Bending Primordial Trajectories Away From Heart Failure.J Am Soc Echocardiogr. 2021 Apr;34(4):401-404. doi: 10.1016/j.echo.2021.01.011. Epub 2021 Jan 13. J Am Soc Echocardiogr. 2021. PMID: 33453368 Free PMC article. No abstract available.
References
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, et al. 2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults. J Am Coll Cardiol. 2009;53(15):e1–e90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
