

Targeting Telomerase with an HLA Class II-Restricted TCR for Cancer Immunotherapy
- PMID: 33212301
- PMCID: PMC7934585
- DOI: 10.1016/j.ymthe.2020.11.019
Targeting Telomerase with an HLA Class II-Restricted TCR for Cancer Immunotherapy
Abstract
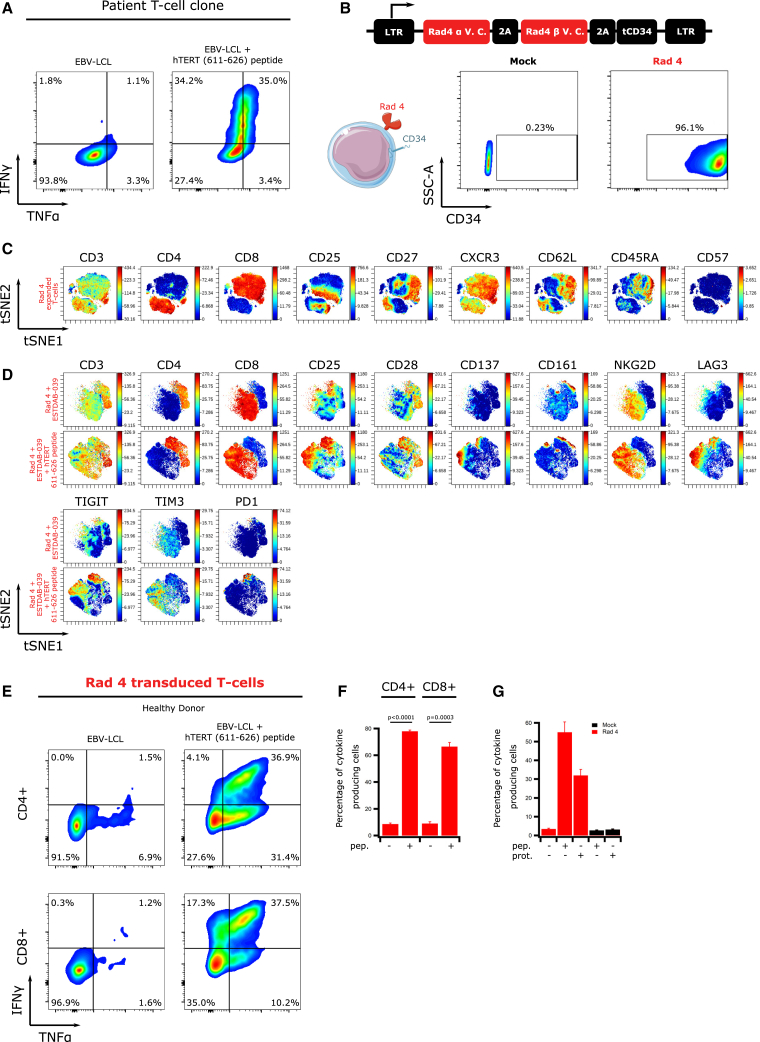
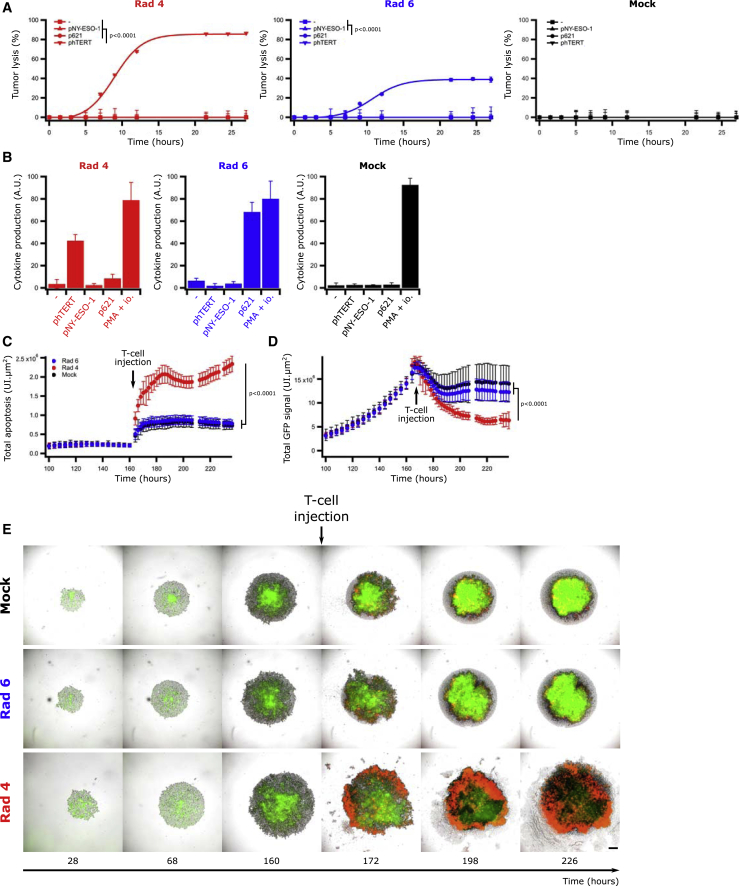
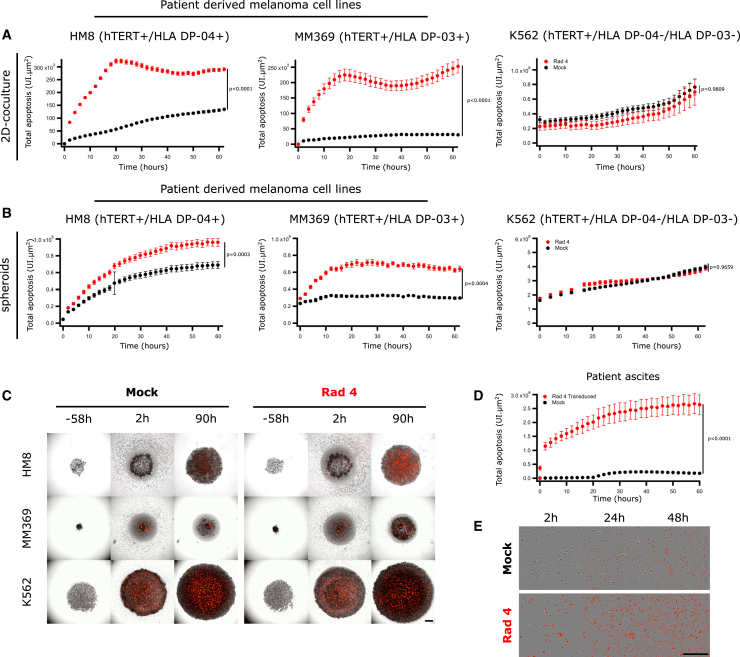
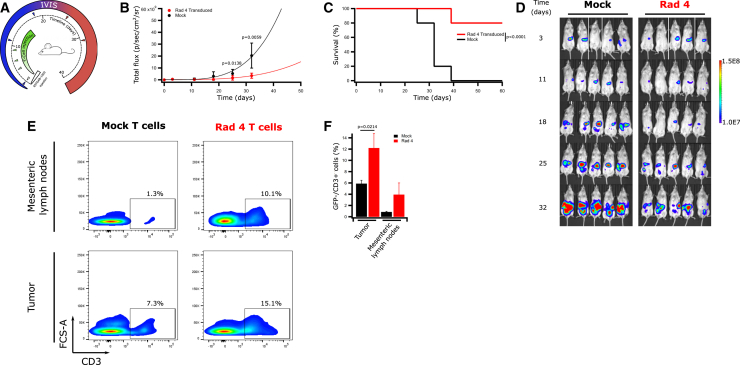
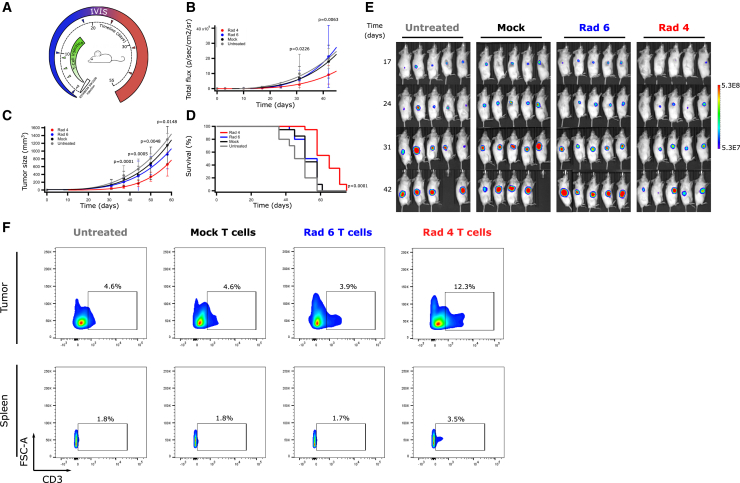
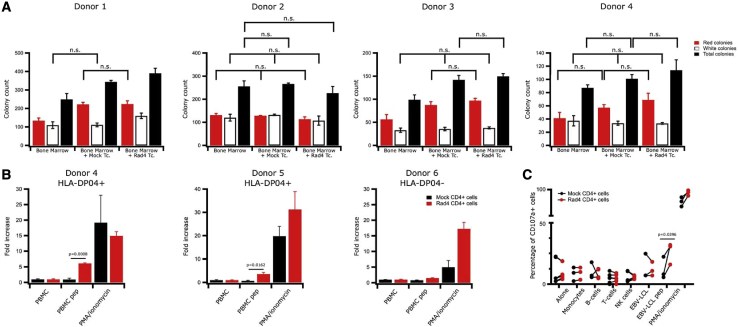
T cell receptor (TCR)-engineered T cell therapy is a promising cancer treatment approach. Human telomerase reverse transcriptase (hTERT) is overexpressed in the majority of tumors and a potential target for adoptive cell therapy. We isolated a novel hTERT-specific TCR sequence, named Radium-4, from a clinically responding pancreatic cancer patient vaccinated with a long hTERT peptide. Radium-4 TCR-redirected primary CD4+ and CD8+ T cells demonstrated in vitro efficacy, producing inflammatory cytokines and killing hTERT+ melanoma cells in both 2D and 3D settings, as well as malignant, patient-derived ascites cells. Importantly, T cells expressing Radium-4 TCR displayed no toxicity against bone marrow stem cells or mature hematopoietic cells. Notably, Radium-4 TCR+ T cells also significantly reduced tumor growth and improved survival in a xenograft mouse model. Since hTERT is a universal cancer antigen, and the very frequently expressed HLA class II molecules presenting the hTERT peptide to this TCR provide a very high (>75%) population coverage, this TCR represents an attractive candidate for immunotherapy of solid tumors.
Keywords: CD4 T cell; MHC class II; T cell receptor; immunotherapy; in vivo model; solid tumor; telomerase.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
G.G., G.K., S.W., and E.M.I. are inventors on the patent WO2019166463. G.G. and G.K. are shareholders in Zelluna Immunotherapy AS. S.P. is currently employed by Zelluna Immunotherapy AS. All other authors declare no competing interests.
Figures

Similar articles
-
A phase I/II escalation trial design T-RAD: Treatment of metastatic lung cancer with mRNA-engineered T cells expressing a T cell receptor targeting human telomerase reverse transcriptase (hTERT).Front Oncol. 2022 Nov 10;12:1031232. doi: 10.3389/fonc.2022.1031232. eCollection 2022. Front Oncol. 2022. PMID: 36439452 Free PMC article.
-
Human melanoma immunotherapy using tumor antigen-specific T cells generated in humanized mice.Oncotarget. 2016 Feb 9;7(6):6448-59. doi: 10.18632/oncotarget.7044. Oncotarget. 2016. PMID: 26824989 Free PMC article.
-
Development of a novel redirected T-cell-based adoptive immunotherapy targeting human telomerase reverse transcriptase for adult T-cell leukemia.Blood. 2013 Jun 13;121(24):4894-901. doi: 10.1182/blood-2012-11-465971. Epub 2013 May 2. Blood. 2013. PMID: 23641014 Clinical Trial.
-
Potential use of T cell receptor genes to modify hematopoietic stem cells for the gene therapy of cancer.Pathol Oncol Res. 1999;5(1):3-15. doi: 10.1053/paor.1999.0003. Pathol Oncol Res. 1999. PMID: 10079371 Review.
-
Recent Advances in Targeting CD8 T-Cell Immunity for More Effective Cancer Immunotherapy.Front Immunol. 2018 Jan 22;9:14. doi: 10.3389/fimmu.2018.00014. eCollection 2018. Front Immunol. 2018. PMID: 29403496 Free PMC article. Review.
Cited by
-
Clinical research progress of telomerase targeted cancer immunotherapy: a literature review.Transl Cancer Res. 2024 Jul 31;13(7):3904-3921. doi: 10.21037/tcr-24-196. Epub 2024 Jul 17. Transl Cancer Res. 2024. PMID: 39145070 Free PMC article. Review.
-
ALPL-1 is a target for chimeric antigen receptor therapy in osteosarcoma.Nat Commun. 2023 Jun 8;14(1):3375. doi: 10.1038/s41467-023-39097-x. Nat Commun. 2023. PMID: 37291203 Free PMC article.
-
Telomerase as a Target for Therapeutic Cancer Vaccines and Considerations for Optimizing Their Clinical Potential.Front Immunol. 2021 Jul 5;12:682492. doi: 10.3389/fimmu.2021.682492. eCollection 2021. Front Immunol. 2021. PMID: 34290704 Free PMC article. Review.
-
A phase I/II escalation trial design T-RAD: Treatment of metastatic lung cancer with mRNA-engineered T cells expressing a T cell receptor targeting human telomerase reverse transcriptase (hTERT).Front Oncol. 2022 Nov 10;12:1031232. doi: 10.3389/fonc.2022.1031232. eCollection 2022. Front Oncol. 2022. PMID: 36439452 Free PMC article.
-
The screening, identification, design and clinical application of tumor-specific neoantigens for TCR-T cells.Mol Cancer. 2023 Aug 30;22(1):141. doi: 10.1186/s12943-023-01844-5. Mol Cancer. 2023. PMID: 37649123 Free PMC article. Review.
References
-
- Lee D.W., Kochenderfer J.N., Stetler-Stevenson M., Cui Y.K., Delbrook C., Feldman S.A., Fry T.J., Orentas R., Sabatino M., Shah N.N. T cells expressing CD19 chimeric antigen receptors for acute lymphoblastic leukaemia in children and young adults: a phase 1 dose-escalation trial. Lancet. 2015;385:517–528. - PMC - PubMed
-
- Zanetti M. A second chance for telomerase reverse transcriptase in anticancer immunotherapy. Nat. Rev. Clin. Oncol. 2017;14:115–128. - PubMed
-
- Harley C.B., Kim N.W., Prowse K.R., Weinrich S.L., Hirsch K.S., West M.D., Bacchetti S., Hirte H.W., Counter C.M., Greider C.W. Telomerase, cell immortality, and cancer. Cold Spring Harb. Symp. Quant. Biol. 1994;59:307–315. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
