

Effects of Canagliflozin in Patients with Baseline eGFR <30 ml/min per 1.73 m2: Subgroup Analysis of the Randomized CREDENCE Trial
- PMID: 33214158
- PMCID: PMC7769025
- DOI: 10.2215/CJN.10140620
Effects of Canagliflozin in Patients with Baseline eGFR <30 ml/min per 1.73 m2: Subgroup Analysis of the Randomized CREDENCE Trial
Abstract
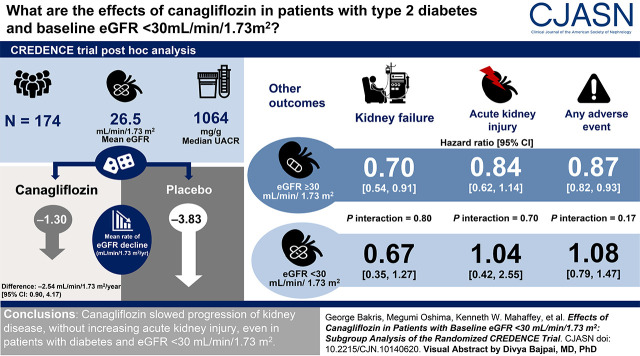
Background and objectives: The Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) trial demonstrated that the sodium glucose cotransporter 2 (SGLT2) inhibitor canagliflozin reduced the risk of kidney failure and cardiovascular events in participants with type 2 diabetes mellitus and CKD. Little is known about the use of SGLT2 inhibitors in patients with eGFR <30 ml/min per 1.73 m2. The participants in the CREDENCE study had type 2 diabetes mellitus, a urinary albumin-creatinine ratio >300-5000 mg/g, and an eGFR of 30 to <90 ml/min per 1.73 m2 at screening. This post hoc analysis evaluated participants with eGFR <30 ml/min per 1.73 m2 at randomization.
Design, setting, participants, & measurements: Effects of eGFR slope through week 130 were analyzed using a piecewise, linear, mixed-effects model. Efficacy was analyzed in the intention-to-treat population, on the basis of Cox proportional hazard models, and safety was analyzed in the on-treatment population. At randomization (an average of 29 days after screening), 174 of 4401 (4%) participants had an eGFR <30 ml/min per 1.73 m2 (mean [SD] eGFR, 26 [3] ml/min per 1.73 m2).
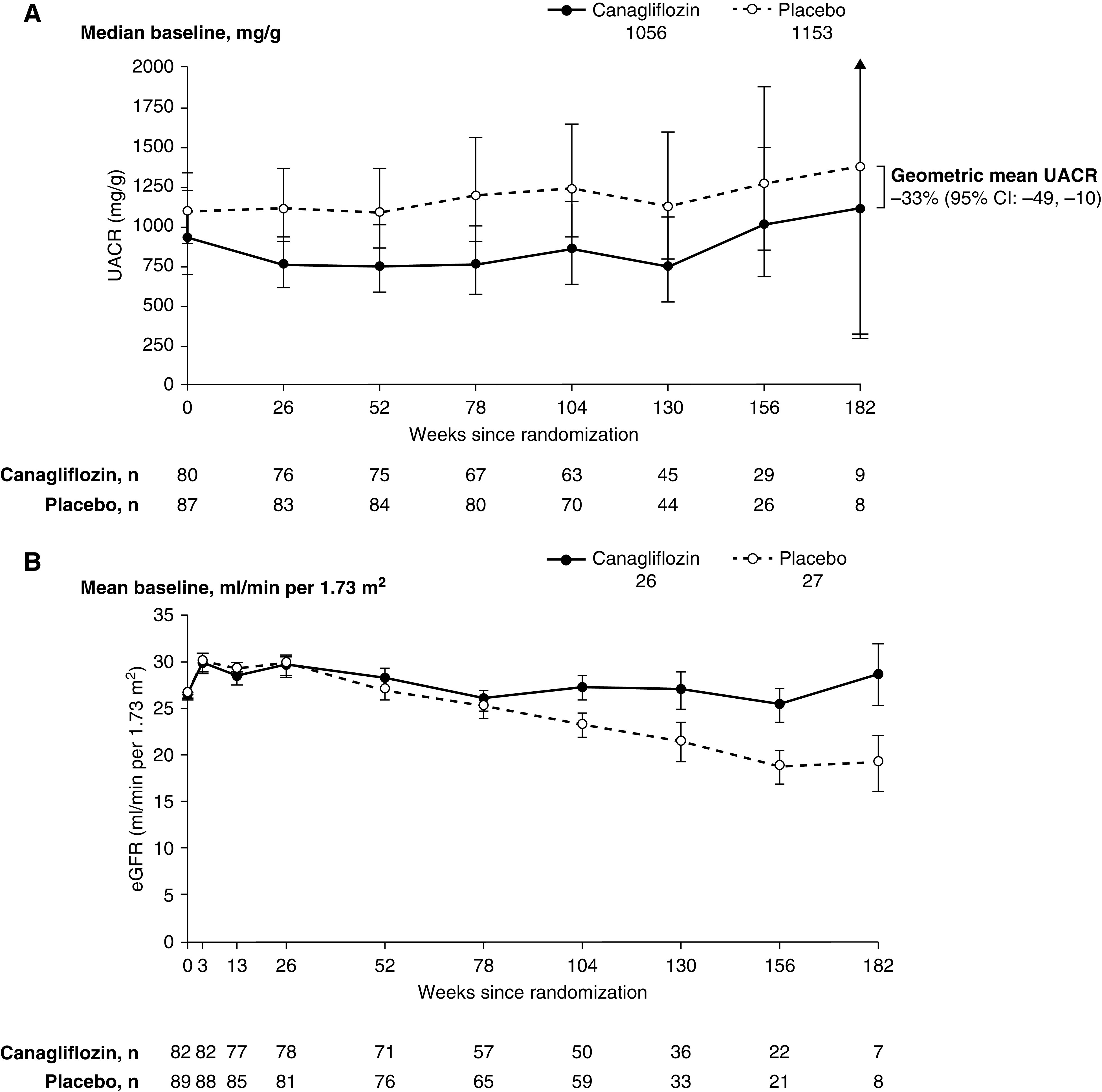
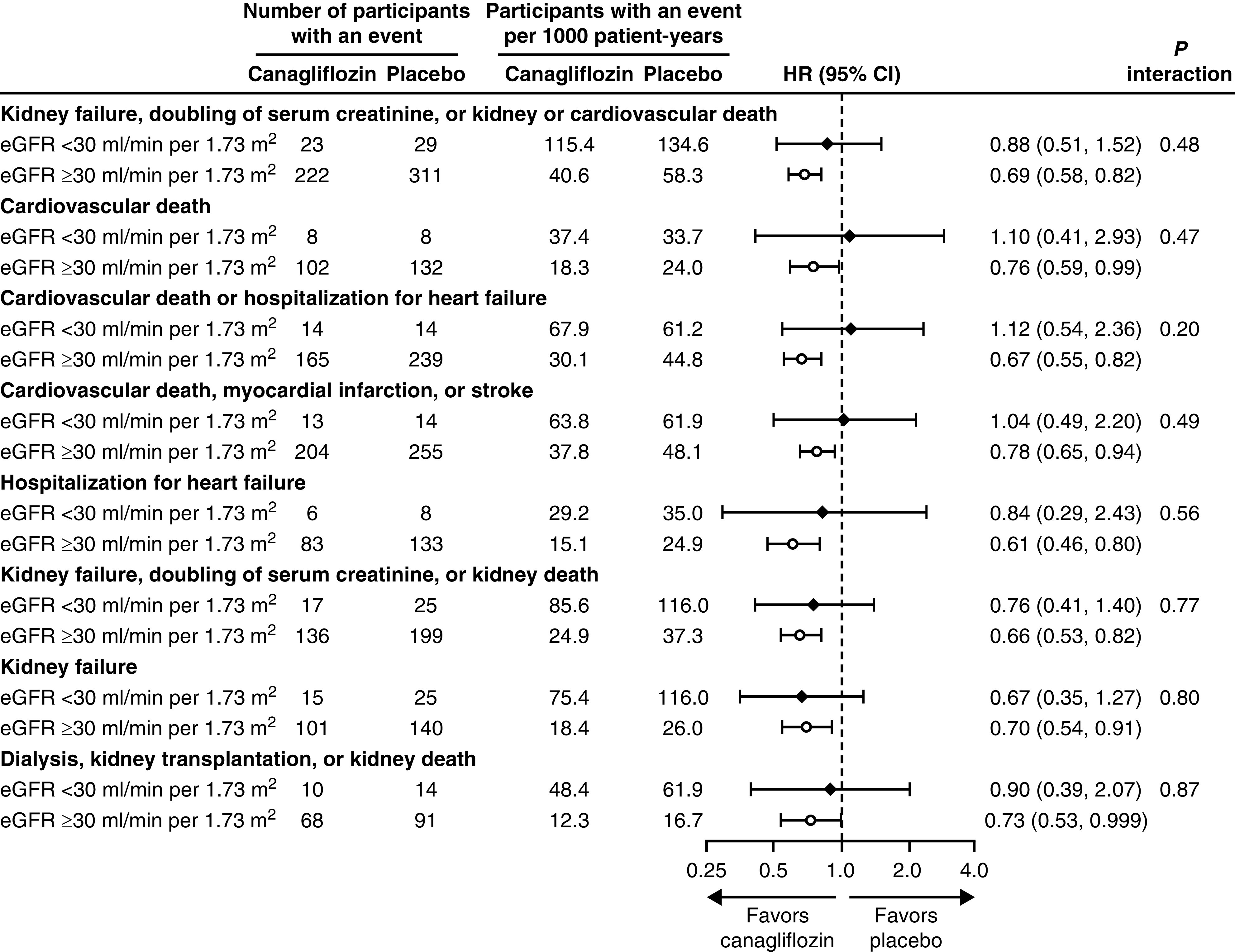
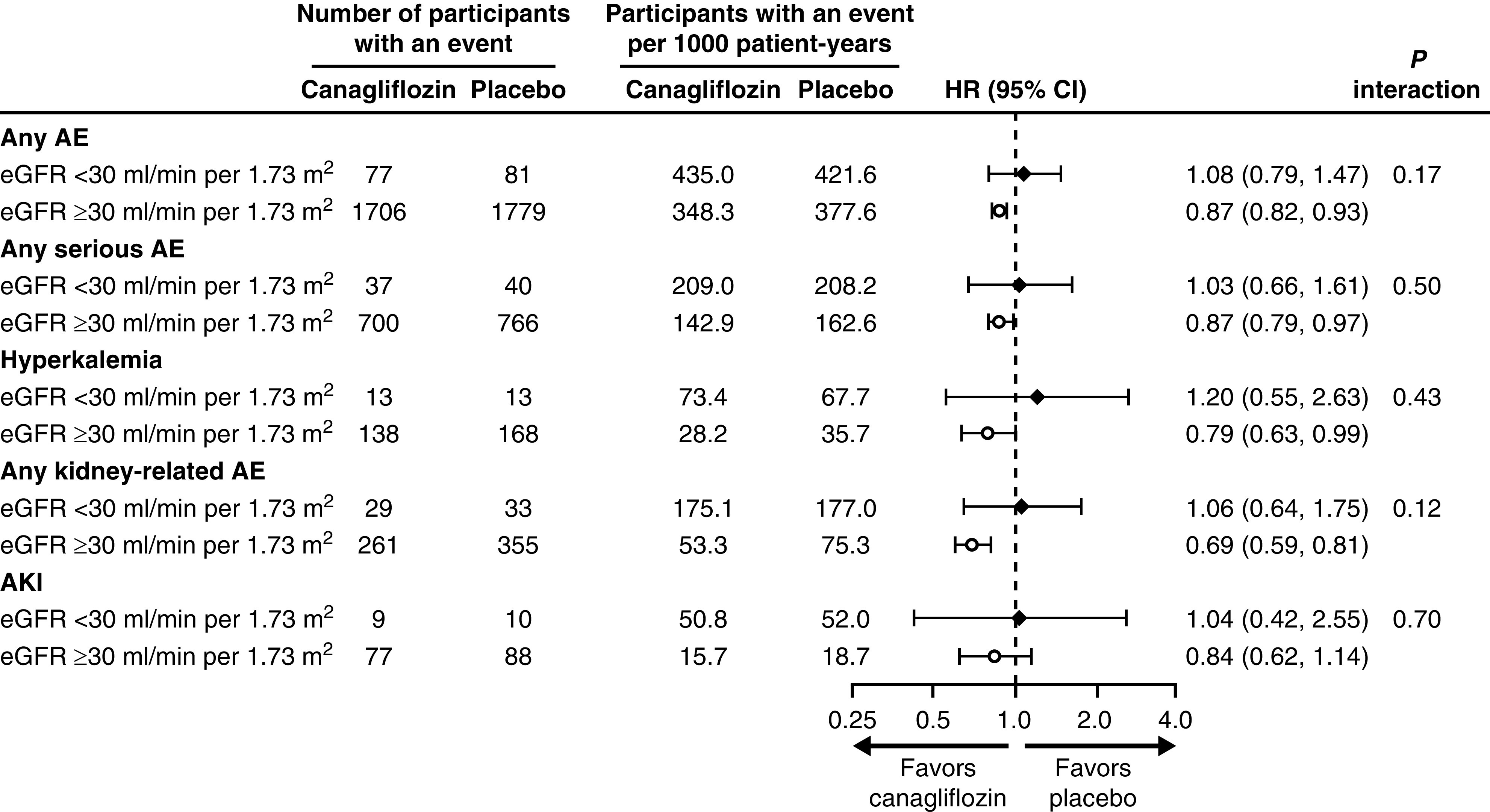
Results: From weeks 3 to 130, there was a 66% difference in the mean rate of eGFR decline with canagliflozin versus placebo (mean slopes, -1.30 versus -3.83 ml/min per 1.73 m2 per year; difference, -2.54 ml/min per 1.73 m2 per year; 95% confidence interval [CI], 0.90 to 4.17). Effects of canagliflozin on kidney, cardiovascular, and mortality outcomes were consistent for those with eGFR <30 and ≥30 ml/min per 1.73 m2 (all P interaction >0.20). The estimate for kidney failure in participants with eGFR <30 ml/min per 1.73 m2 (hazard ratio, 0.67; 95% CI, 0.35 to 1.27) was similar to those with eGFR ≥30 ml/min per 1.73 m2 (hazard ratio, 0.70; 95% CI, 0.54 to 0.91; P interaction=0.80). There was no imbalance in the rate of kidney-related adverse events or AKI associated with canagliflozin between participants with eGFR <30 and ≥30 ml/min per 1.73 m2 (all P interaction >0.12).
Conclusions: This post hoc analysis suggests canagliflozin slowed progression of kidney disease, without increasing AKI, even in participants with eGFR <30 ml/min per 1.73 m2.
Keywords: canagliflozin; chronic kidney disease; diabetes; diabetic nephropathy.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
Are SGLT2 Inhibitors Safe and Effective in Advanced Diabetic Kidney Disease?Clin J Am Soc Nephrol. 2020 Dec 7;15(12):1694-1695. doi: 10.2215/CJN.16351020. Epub 2020 Nov 19. Clin J Am Soc Nephrol. 2020. PMID: 33214159 Free PMC article. No abstract available.
References
-
- Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S; RENAAL Study Investigators: Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345: 861–869, 2001 - PubMed
-
- Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, Ritz E, Atkins RC, Rohde R, Raz I; Collaborative Study Group: Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 345: 851–860, 2001 - PubMed
-
- Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Furtado RHM, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Sabatine MS: SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet 393: 31–39, 2019 - PubMed
-
- Jardine MJ, Mahaffey KW, Neal B, Agarwal R, Bakris GL, Brenner BM, Bull S, Cannon CP, Charytan DM, de Zeeuw D, Edwards R, Greene T, Heerspink HJL, Levin A, Pollock C, Wheeler DC, Xie J, Zhang H, Zinman B, Desai M, Perkovic V; CREDENCE study investigators : The Canagliflozin and Renal Endpoints in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) study rationale, design, and baseline characteristics. Am J Nephrol 46: 462–472, 2017. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
