

Solving the problem of access to cardiovascular medicines: revolving fund pharmacy models in rural western Kenya
- PMID: 33214173
- PMCID: PMC7678234
- DOI: 10.1136/bmjgh-2020-003116
Solving the problem of access to cardiovascular medicines: revolving fund pharmacy models in rural western Kenya
Abstract
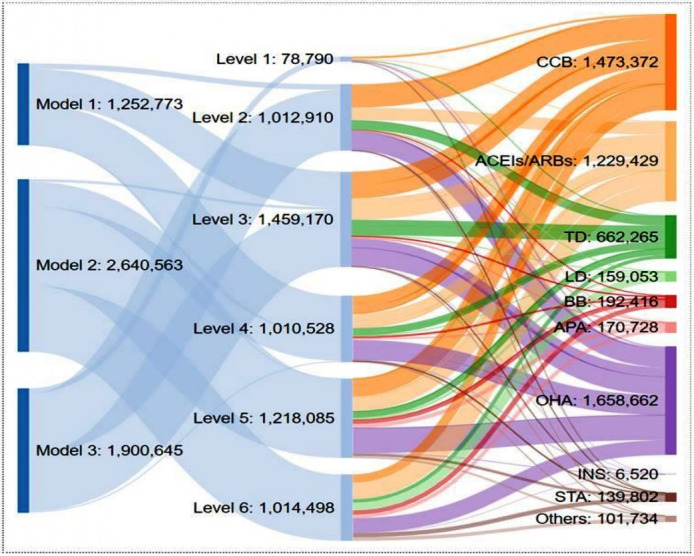
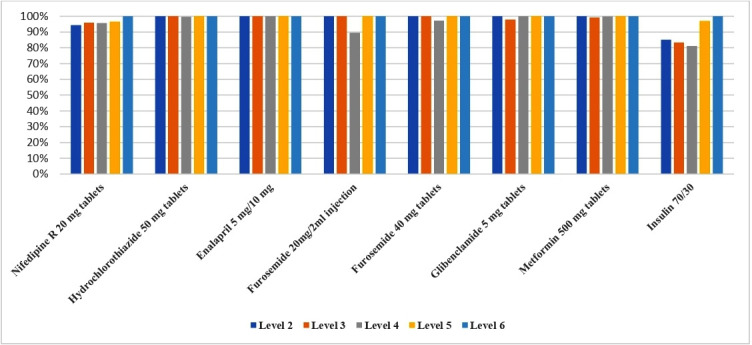
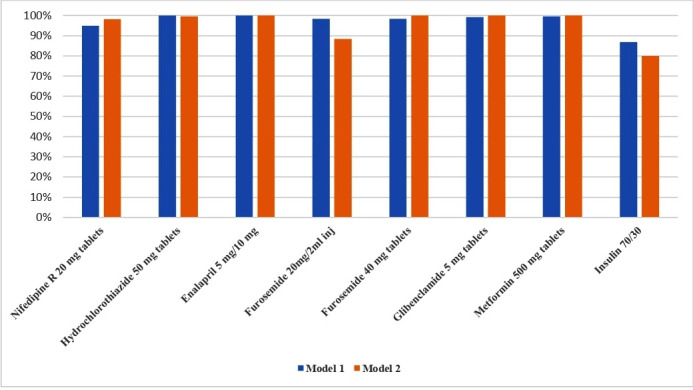
Availability of medicines for treatment of cardiovascular disease (CVD) is low in low-income and middle-income countries (LMIC). Supply chain models to improve the availability of quality CVD medicines in LMIC communities are urgently required. Our team established contextualised revolving fund pharmacies (RFPs) in rural western Kenya, whereby an initial stock of essential medicines was obtained through donations or purchase and then sold at a small mark-up price sufficient to replenish drug stock and ensure sustainability. In response to different contexts and levels of the public health system in Kenya (eg, primary versus tertiary), we developed and implemented three contextualised models of RFPs over the past decade, creating a network of 72 RFPs across western Kenya, that supplied 22 categories of CVD medicines and increased availability of essential CVD medications from <30% to 90% or higher. In one representative year, we were able to successfully supply 5 793 981 units of CVD and diabetes medicines to patients in western Kenya. The estimated programme running cost was US$6.5-25 per patient, serving as a useful benchmark for public governments to invest in medication supply chain systems in LMICs going forward. One important lesson that we have learnt from implementing three different RFP models over the past 10 years has been that each model has its own advantages and disadvantages, and we must continue to stay nimble and modify as needed to determine the optimal supply chain model while ensuring consistent access to essential CVD medications for patients living in these settings.
Keywords: cardiovascular disease; descriptive study; diabetes; health services research.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Sonak Pastakia serves as a consultant for Abbott and Becton Dickinson on work unrelated to the study being presented here. The other authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous