

Distinct immunologic endotypes are associated with clinical trajectory after severe blunt trauma and hemorrhagic shock
- PMID: 33214489
- PMCID: PMC8194286
- DOI: 10.1097/TA.0000000000003029
Distinct immunologic endotypes are associated with clinical trajectory after severe blunt trauma and hemorrhagic shock
Abstract
Background: The genomic/cytokine "storm" after severe trauma is well described. However, the differing composition, magnitude and resolution of this response, and its relationship to clinical outcomes remain unclear.
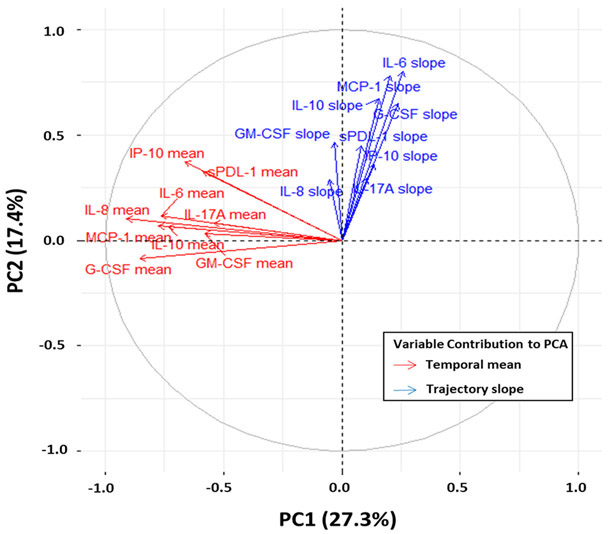
Methods: This is a secondary analysis of a prospective longitudinal cohort study of severely injured trauma patients in hemorrhagic shock. Peripheral blood sampling was performed at 0.5, 1, 4, 7, 14, and 28 days after injury for measurement of circulating immune biomarkers. K-means clustering using overall mean and trajectory slope of selected immunologic biomarkers were used to identify distinct temporal immunologic endotypes. Endotypes were compared with known clinical trajectories defined as early death (<14 days), chronic critical illness (CCI) (ICU length of stay of ≥14 days with persistent organ dysfunction), and rapid recovery (RAP) (ICU length of stay of <14 days with organ recovery).
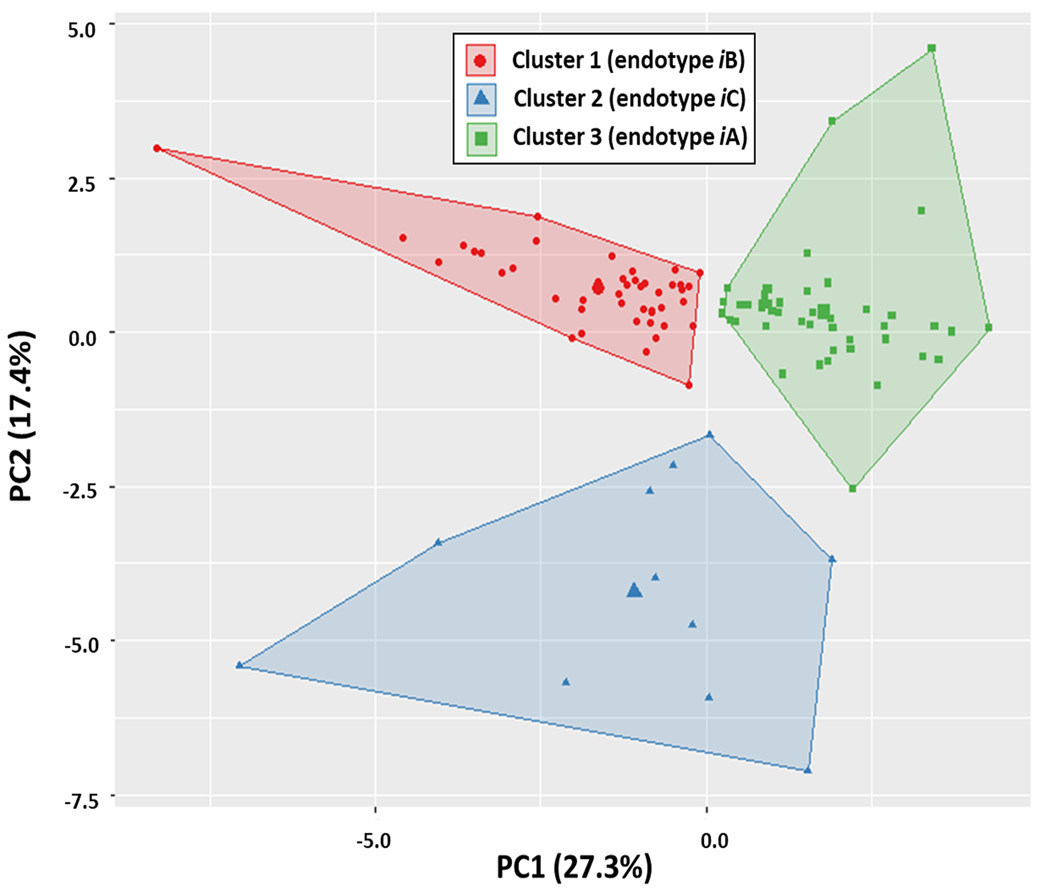
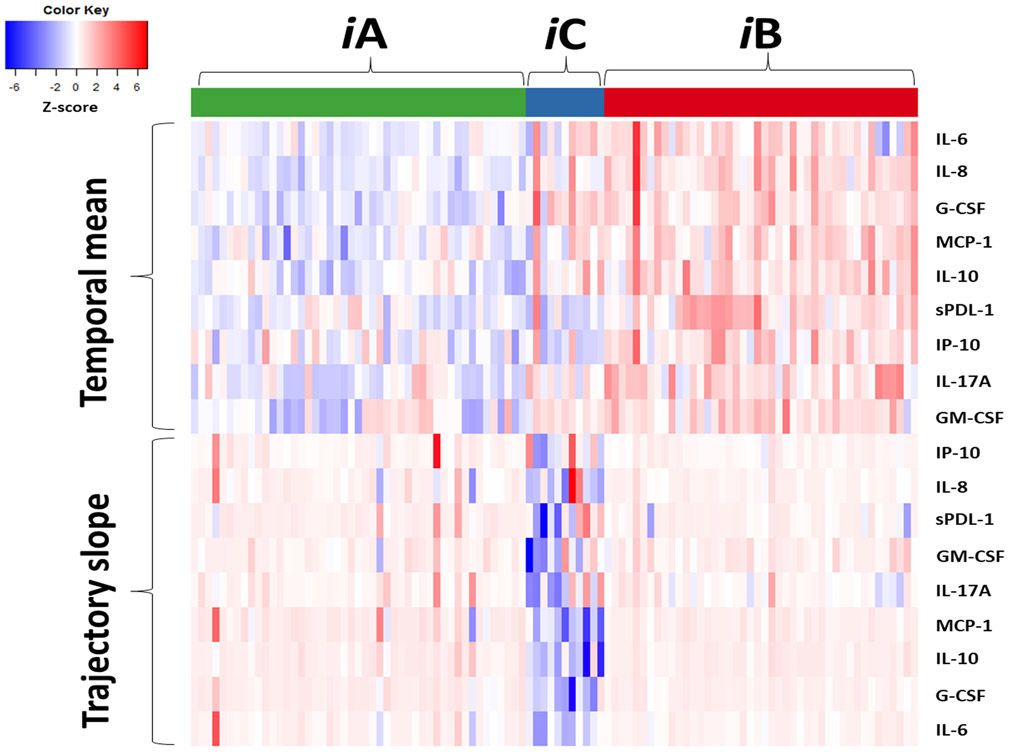
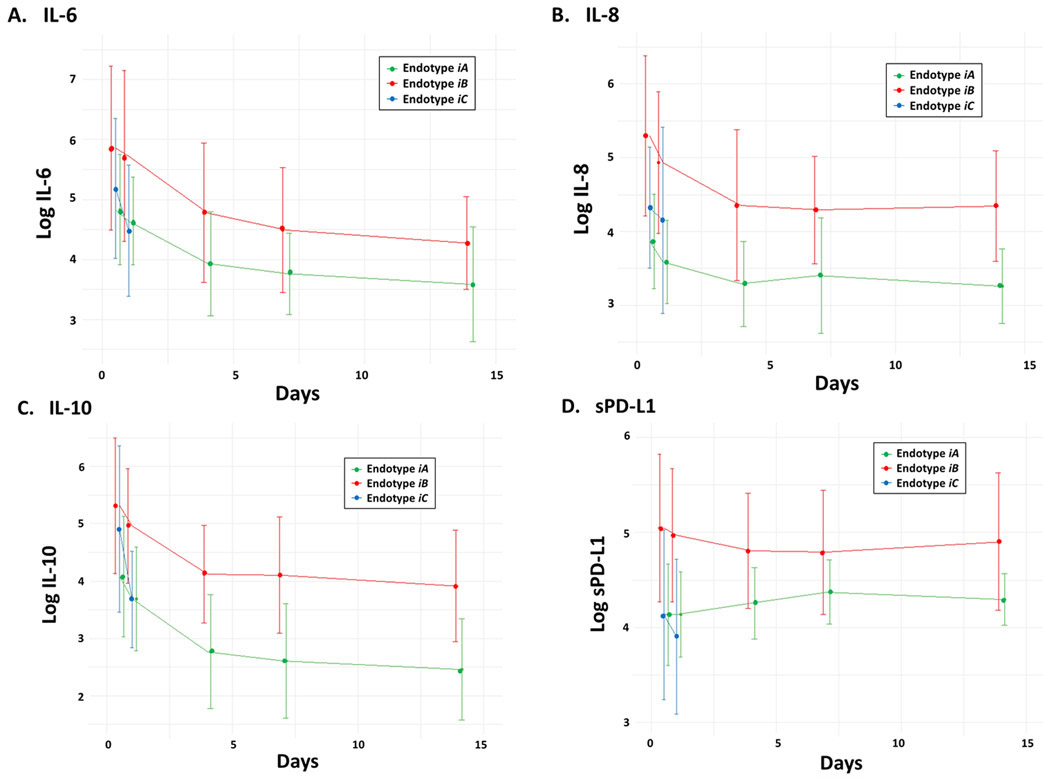
Results: The cohort included 102 subjects enrolled across 2 level 1 trauma centers. We identified three distinct immunologic endotypes (iA, iB, and iC), each with unique associations to clinical trajectory. Endotype iA (n = 47) exhibited a moderate initial proinflammatory response followed by a return to immunologic homeostasis, with a primary clinical trajectory of RAP (n = 44, 93.6%). Endotype iB (n = 44) exhibited an early hyperinflammatory response with persistent inflammation and immunosuppression, with the highest incidence of CCI (n = 10, 22.7%). Endotype iC (n = 11) exhibited a similar hyperinflammatory response, but with rapid return to immunologic homeostasis and a predominant trajectory of RAP (n = 9, 81.8%). Patients with endotype iB had the highest severity/duration of organ dysfunction and highest incidence of nosocomial infections (50%, p = 0.001), and endotype iB was the predominant endotype of patients who developed CCI (10 of 13 patients, 76.9%; p = 0.002).
Conclusion: We identified three distinct immunologic endotypes after severe injury differing the magnitude and duration of the early response. The clinical trajectory of CCI is characterized by an endotype (iB) defined by persistent alteration in inflammation/immunosuppression and is associated with poor clinical outcomes.
Level of evidence: Prognostic, level III.
Trial registration: ClinicalTrials.gov NCT01810328.
Copyright © 2020 American Association for the Surgery of Trauma.
Figures
References
-
- Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471–82. - PMC - PubMed
-
- Ciesla DJ, Moore EE, Johnson JL, Burch JM, Cothren CC, Sauaia A. A 12-year prospective study of postinjury multiple organ failure: has anything changed? Arch Surg. 2005;140(5):432–8; discussion 8-40. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
