

Systematic review of clinical effectiveness, components, and delivery of pulmonary rehabilitation in low-resource settings
- PMID: 33214560
- PMCID: PMC7677536
- DOI: 10.1038/s41533-020-00210-y
Systematic review of clinical effectiveness, components, and delivery of pulmonary rehabilitation in low-resource settings
Abstract
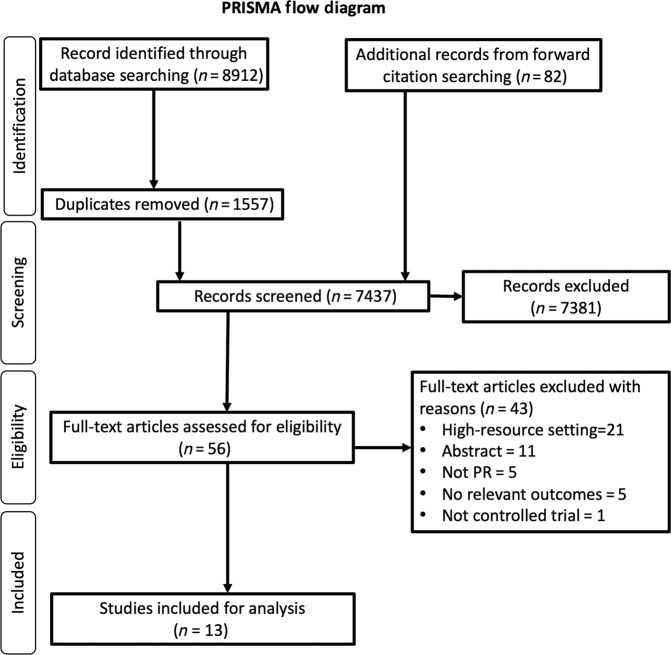
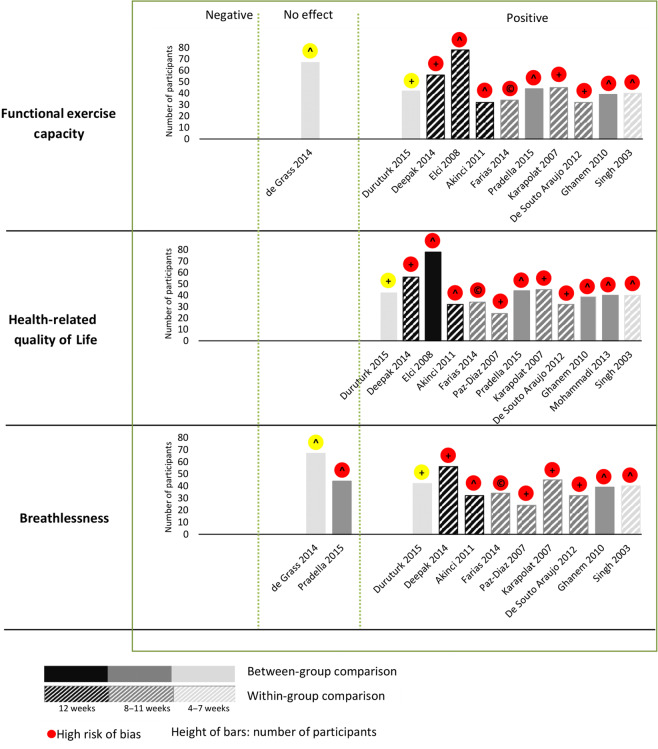
Pulmonary rehabilitation (PR) is a guideline-recommended multifaceted intervention that improves the physical and psychological well-being of people with chronic respiratory diseases (CRDs), though most of the evidence derives from trials in high-resource settings. In low- and middle-income countries, PR services are under-provided. We aimed to review the effectiveness, components and mode of delivery of PR in low-resource settings. Following Cochrane methodology, we systematically searched (1990 to October 2018; pre-publication update March 2020) MEDLINE, EMBASE, CABI, AMED, PUBMED, and CENTRAL for controlled clinical trials of adults with CRD (including but not restricted to chronic obstructive pulmonary disease) comparing PR with usual care in low-resource settings. After duplicate selection, we extracted data on exercise tolerance, health-related quality of life (HRQoL), breathlessness, included components, and mode of delivery. We used Cochrane risk of bias (RoB) to assess study quality and synthesised data narratively. From 8912 hits, we included 13 studies: 11 were at high RoB; 2 at moderate RoB. PR improved functional exercise capacity in 10 studies, HRQoL in 12, and breathlessness in 9 studies. One of the two studies at moderate RoB showed no benefit. All programmes included exercise training; most provided education, chest physiotherapy, and breathing exercises. Low cost services, adapted to the setting, used limited equipment and typically combined outpatient/centre delivery with a home/community-based service. Multicomponent PR programmes can be delivered in low-resource settings, employing a range of modes of delivery. There is a need for a high-quality trial to confirm the positive findings of these high/moderate RoB studies.
Conflict of interest statement
Neither the funder nor the sponsor (University of Edinburgh) contributed to protocol development. G.M.M.H. owns a pulmonary rehabilitation clinic in Bangladesh. All other authors declare no competing interests.
Figures
Similar articles
-
Active mind-body movement therapies as an adjunct to or in comparison with pulmonary rehabilitation for people with chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2018 Oct 10;10(10):CD012290. doi: 10.1002/14651858.CD012290.pub2. Cochrane Database Syst Rev. 2018. PMID: 30306545 Free PMC article.
-
Systematic review (protocol) of clinical effectiveness and models of care of low-resource pulmonary rehabilitation.NPJ Prim Care Respir Med. 2019 Apr 5;29(1):10. doi: 10.1038/s41533-019-0122-1. NPJ Prim Care Respir Med. 2019. PMID: 30952884 Free PMC article.
-
Telerehabilitation for chronic respiratory disease.Cochrane Database Syst Rev. 2021 Jan 29;1(1):CD013040. doi: 10.1002/14651858.CD013040.pub2. Cochrane Database Syst Rev. 2021. PMID: 33511633 Free PMC article.
-
Clinical effectiveness and components of Home-pulmonary rehabilitation for people with chronic respiratory diseases: a systematic review protocol.BMJ Open. 2021 Oct 12;11(10):e050362. doi: 10.1136/bmjopen-2021-050362. BMJ Open. 2021. PMID: 34642195 Free PMC article.
-
Physiotherapy rehabilitation after total knee or hip replacement: an evidence-based analysis.Ont Health Technol Assess Ser. 2005;5(8):1-91. Epub 2005 Jun 1. Ont Health Technol Assess Ser. 2005. PMID: 23074477 Free PMC article.
Cited by
-
Perspectives of Patients With Chronic Respiratory Diseases and Medical Professionals on Pulmonary Rehabilitation in Pune, India: Qualitative Analysis.JMIR Form Res. 2023 Nov 7;7:e45624. doi: 10.2196/45624. JMIR Form Res. 2023. PMID: 37934558 Free PMC article.
-
Protocol for a single-centre mixed-method pre-post single-arm feasibility trial of a culturally appropriate 6-week pulmonary rehabilitation programme among adults with functionally limiting chronic respiratory diseases in Malawi.BMJ Open. 2022 Jan 31;12(1):e057538. doi: 10.1136/bmjopen-2021-057538. BMJ Open. 2022. PMID: 35105655 Free PMC article.
-
Feasibility of a pulmonary rehabilitation programme for patients with symptomatic chronic obstructive pulmonary disease in Georgia: a single-site, randomised controlled trial from the Breathe Well Group.BMJ Open. 2022 Sep 23;12(9):e056902. doi: 10.1136/bmjopen-2021-056902. BMJ Open. 2022. PMID: 36153030 Free PMC article. Clinical Trial.
-
Greater exercise tolerance in COPD during acute intermittent compared to continuous shuttle walking protocols: A proof-of-concept study.Chron Respir Dis. 2022 Jan-Dec;19:14799731221142023. doi: 10.1177/14799731221142023. Chron Respir Dis. 2022. PMID: 36548147 Free PMC article.
-
Developing Appropriate Pulmonary Rehabilitation Services in Sri Lanka: Assessment of People Living with COPD and Healthcare Providers in Urban and Semi Urban Areas in Sri Lanka.Int J Chron Obstruct Pulmon Dis. 2022 Mar 25;17:631-641. doi: 10.2147/COPD.S316555. eCollection 2022. Int J Chron Obstruct Pulmon Dis. 2022. PMID: 35386389 Free PMC article.
References
-
- World Health Organisation. Global alliance against chronic respiratory diseases. Global surveillance, prevention and control of chronic respiratory diseases. A comprehensive approach. https://www.who.int/respiratory/en/ (2007).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
