

Applicability of the WHO maternal near-miss tool: A nationwide surveillance study in Suriname
- PMID: 33214899
- PMCID: PMC7649043
- DOI: 10.7189/jogh.10.020429
Applicability of the WHO maternal near-miss tool: A nationwide surveillance study in Suriname
Abstract
Background: Maternal near-miss (MNM) is an important maternal health quality-of-care indicator. To facilitate comparison between countries, the World Health Organization (WHO) developed the "MNM-tool". However, several low- and middle-income countries have proposed adaptations to prevent underreporting, ie, Namibian and Sub-Sahara African (SSA)-criteria. This study aims to assess MNM and associated factors in middle-income country Suriname by applying the three different MNM tools.
Methods: A nationwide prospective population-based cohort study was conducted using the Suriname Obstetric Surveillance System (SurOSS). We included women with MNM-criteria defined by WHO-, Namibian- and SSA-tools during one year (March 2017-February 2018) and used hospital births (86% of total) as a reference group.
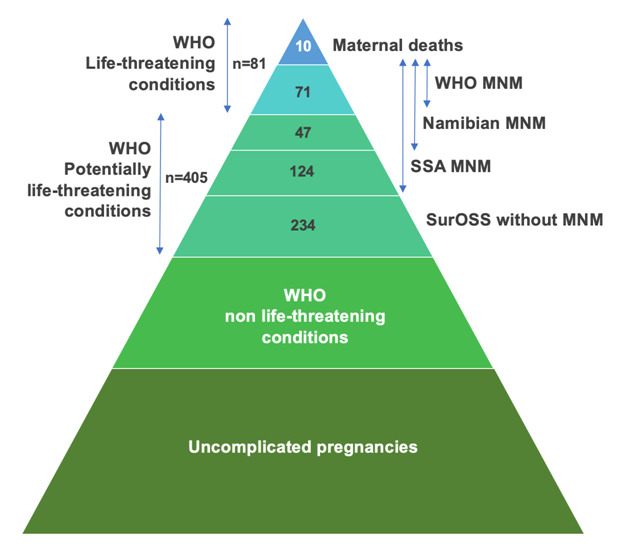
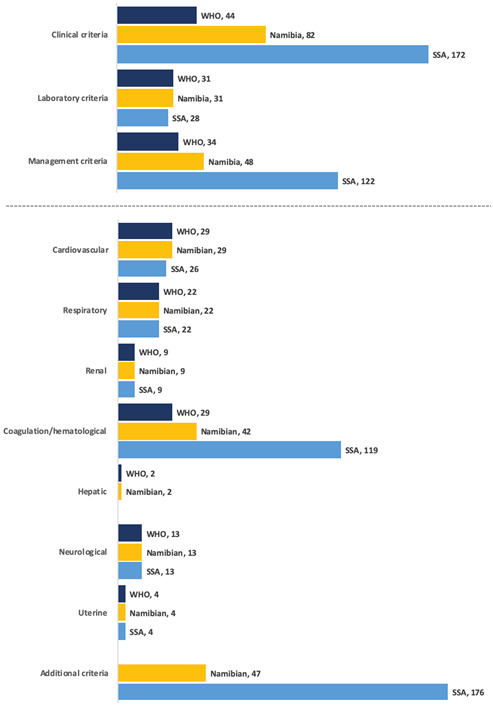
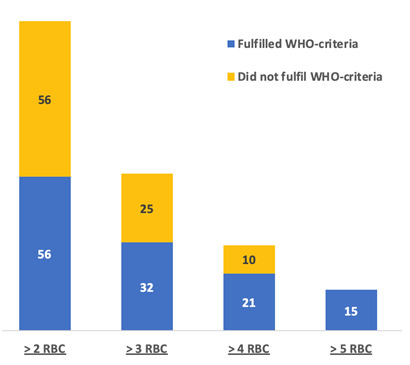
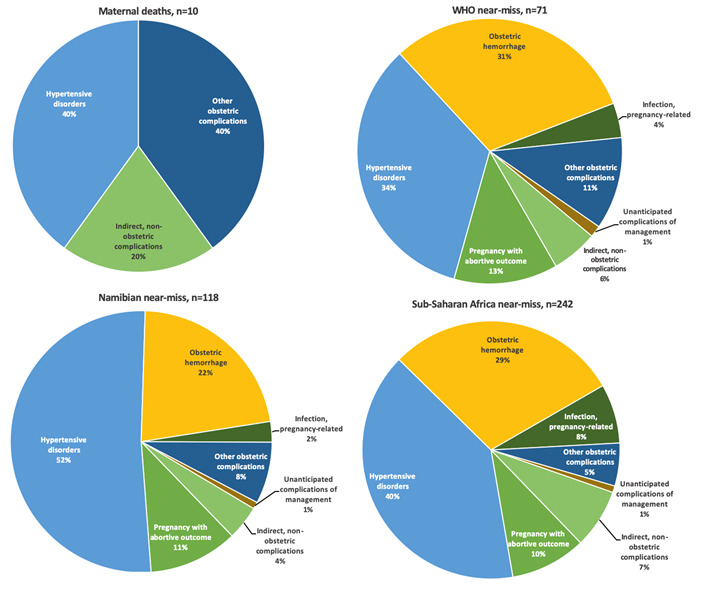
Results: There were 9114 hospital live births in Suriname in the one-year study period. SurOSS identified 71 women with WHO-MNM (8/1000 live births, mortality-index 12%), 118 with Namibian-MNM (13/1000 live births, mortality-index 8%), and 242 with SSA-MNM (27/1000 live births, mortality-index 4%). Namibian- and SSA-tools identified all women with WHO-criteria. Blood transfusion thresholds and eclampsia explained the majority of differences in MNM prevalence. Eclampsia was not considered a WHO-MNM in 80% (n = 35/44) of cases. Nevertheless, mortality-index for MNM with hypertensive disorders was 17% and the most frequent underlying cause of maternal deaths (n = 4/10, 40%) and MNM (n = 24/71, 34%). Women of advanced age and maroon ethnicity had twice the odds of WHO-MNM (respectively adjusted odds ratio (aOR) = 2.6, 95% confidence interval (CI) = 1.4-4.8 and aOR = 2.0, 95% CI = 1.2-3.6). The stillbirths rate among women with WHO-MNM was 193/1000births, with six times higher odds than women without MNM (aOR = 6.8, 95%CI = 3.0-15.8). While the prevalence and mortality-index differ between the three MNM tools, the underlying causes of and factors associated with MNM were comparable.
Conclusions: The MNM ratio in Suriname is comparable to other countries in the region. The WHO-tool underestimates the prevalence of MNM (high mortality-index), while the adapted tools may overestimate MNM and compromise global comparability. Contextualized MNM-criteria per obstetric transition stage may improve comparability and reduce underreporting. While MNM studies facilitate international comparison, audit will remain necessary to identify shortfalls in quality-of-care and improve maternal outcomes.
Copyright © 2020 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Competing interests: The authors completed the ICMJE Unified Competing Interest form (available upon request from the corresponding author), and declare no conflicts of interest.
Figures
References
-
- Alkema L, Chou D, Hogan D, Zhang S, Moller A-B, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet. 2016;387:462-74. 10.1016/S0140-6736(15)00838-7 - DOI - PMC - PubMed
-
- World Health Organization. The WHO near-miss approach for maternal health - Evaluating the quality of care for severe pregnancy complications. World Health Organization. 2011. Available: https://apps.who.int/iris/bitstream/handle/10665/44692/9789241502221_eng.... Accessed: 12 December 2019.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
