

Sleep disordered breathing and chronic obstructive pulmonary disease: a narrative review on classification, pathophysiology and clinical outcomes
- PMID: 33214924
- PMCID: PMC7642631
- DOI: 10.21037/jtd-cus-2020-006
Sleep disordered breathing and chronic obstructive pulmonary disease: a narrative review on classification, pathophysiology and clinical outcomes
Abstract
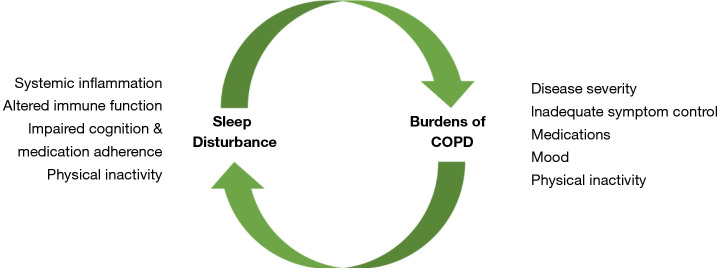
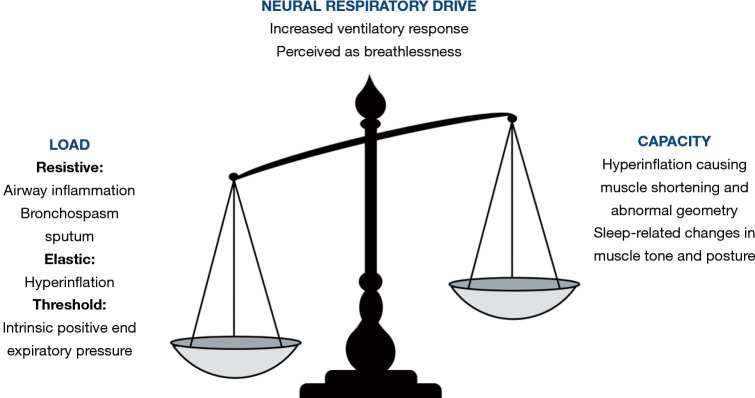
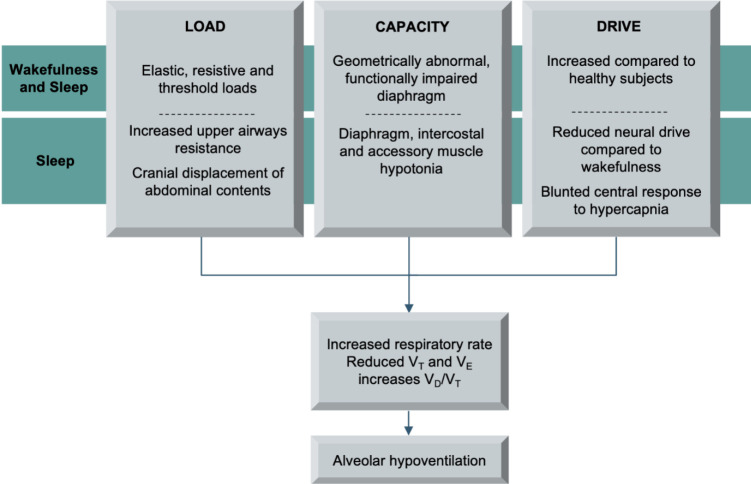
Chronic obstructive pulmonary disease (COPD) causes load-capacity-drive imbalance in both wakefulness and sleep, principally driven by expiratory flow limitation and hyperinflation. Sleep imposes additional burdens to the respiratory muscle pump, driven by changes in respiratory muscle tone, neural respiratory drive and consequences of the supine position. COPD patients are therefore at higher risk of decompensation during sleep, which may manifest as altered sleep architecture, isolated nocturnal desaturation, sleep hypoventilation and restless legs. Each form of sleep disordered breathing in COPD is associated with adverse clinical and patient-reported outcomes, including increased risk of exacerbations, hospitalisation, cardiovascular events, reduced survival and poorer quality of life. COPD-obstructive sleep apnoea (OSA) overlap syndrome represents a distinct clinical diagnosis, in which clinical outcomes are significantly worse than in either disease alone, including increased mortality, risk of cardiovascular events, hospitalisation and exacerbation frequency. Sleep disordered breathing is under-recognised by COPD patients and their clinicians, however early diagnosis and management is crucial to reduce the risk of adverse clinical outcomes. In this narrative review, we describe the pathophysiology of COPD and physiological changes that occur during sleep, manifestations and diagnosis of sleep disordered breathing in COPD and associated clinical outcomes.
Keywords: COPD-obstructive sleep apnoea (OSA) overlap; Chronic obstructive pulmonary disease (COPD); pulmonary mechanics; respiratory physiology; sleep; sleep disordered breathing.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (Available at http://dx.doi.org/10.21037/jtd-cus-2020-006). The series “5th Clinical Update Sleep” was commissioned by the editorial office without any funding or sponsorship. JS served as the unpaid Guest Editor of the series and serves as an unpaid editorial board member of Journal of Thoracic Disease. PBM reports grants and personal fees from Philips, grants and personal fees from ResMed, grants and personal fees from F&P, grants and personal fees from B&D Electromedical, personal fees from Santhera, grants from GSK, outside the submitted work. The authors have no other conflicts of interest to declare.
Figures
Similar articles
-
Sleep disordered breathing: OSA-COPD overlap.Expert Rev Respir Med. 2024 Jun;18(6):369-379. doi: 10.1080/17476348.2024.2373790. Epub 2024 Jul 2. Expert Rev Respir Med. 2024. PMID: 38932721 Review.
-
Chronic obstructive pulmonary disease and obstructive sleep apnoea-the overlap syndrome.J Thorac Dis. 2016 Feb;8(2):236-42. doi: 10.3978/j.issn.2072-1439.2016.01.52. J Thorac Dis. 2016. PMID: 26904264 Free PMC article. Review.
-
Respiratory mechanics and ventilatory control in overlap syndrome and obesity hypoventilation.Respir Res. 2013 Nov 20;14(1):132. doi: 10.1186/1465-9921-14-132. Respir Res. 2013. PMID: 24256627 Free PMC article. Review.
-
Comorbid obstructive sleep apnoea and chronic obstructive pulmonary disease and the risk of cardiovascular disease.J Thorac Dis. 2018 Dec;10(Suppl 34):S4253-S4261. doi: 10.21037/jtd.2018.10.117. J Thorac Dis. 2018. PMID: 30687541 Free PMC article. Review.
-
A review of therapies for the overlap syndrome of obstructive sleep apnea and chronic obstructive pulmonary disease.FASEB Bioadv. 2021 Jun 11;3(9):683-693. doi: 10.1096/fba.2021-00024. eCollection 2021 Sep. FASEB Bioadv. 2021. PMID: 34485837 Free PMC article.
Cited by
-
Sleep medicine: Practice, challenges and new frontiers.Front Neurol. 2022 Oct 14;13:966659. doi: 10.3389/fneur.2022.966659. eCollection 2022. Front Neurol. 2022. PMID: 36313516 Free PMC article. Review.
-
Diagnosis and management of comorbid disease in COPD.Breathe (Sheff). 2025 Feb 25;21(1):240099. doi: 10.1183/20734735.0099-2024. eCollection 2025 Jan. Breathe (Sheff). 2025. PMID: 40007528 Free PMC article. Review.
-
Biomarkers of the L-Arginine/Dimethylarginine/Nitric Oxide Pathway in People with Chronic Airflow Obstruction and Obstructive Sleep Apnoea.J Clin Med. 2023 Aug 11;12(16):5230. doi: 10.3390/jcm12165230. J Clin Med. 2023. PMID: 37629272 Free PMC article.
-
Does testing for sleep-disordered breathing predischarge vs postdischarge result in different treatment outcomes?J Clin Sleep Med. 2021 Dec 1;17(12):2451-2460. doi: 10.5664/jcsm.9450. J Clin Sleep Med. 2021. PMID: 34216199 Free PMC article.
-
Characteristics of the nocturnal desaturation waveform pattern of SpO2 in COPD patients: an observational study.Respir Res. 2021 Oct 26;22(1):276. doi: 10.1186/s12931-021-01868-9. Respir Res. 2021. PMID: 34702275 Free PMC article.
References
-
- World Health Organisation. Projections of mortality and causes of death, 2016 and 2060. Accessed 5th May 2020. Available online: http://www.who.int/healthinfo/global_burden_disease/projections/en/
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources