

Parafoveal retinal massage combined with autologous blood cover in the management of giant, persistent or recurrent macular holes
- PMID: 33215009
- PMCID: PMC7590867
- DOI: 10.18240/ijo.2020.11.14
Parafoveal retinal massage combined with autologous blood cover in the management of giant, persistent or recurrent macular holes
Abstract
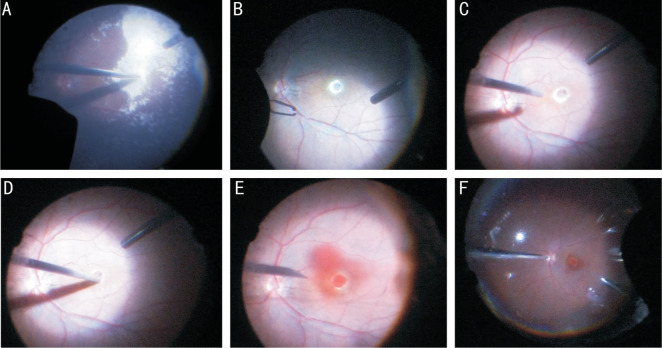
Aim: To assess the efficacy and safety of parafoveal retinal massage combined with autologous whole blood cover in the treatment of refractory macular holes (MHs) and present the surgical procedure.
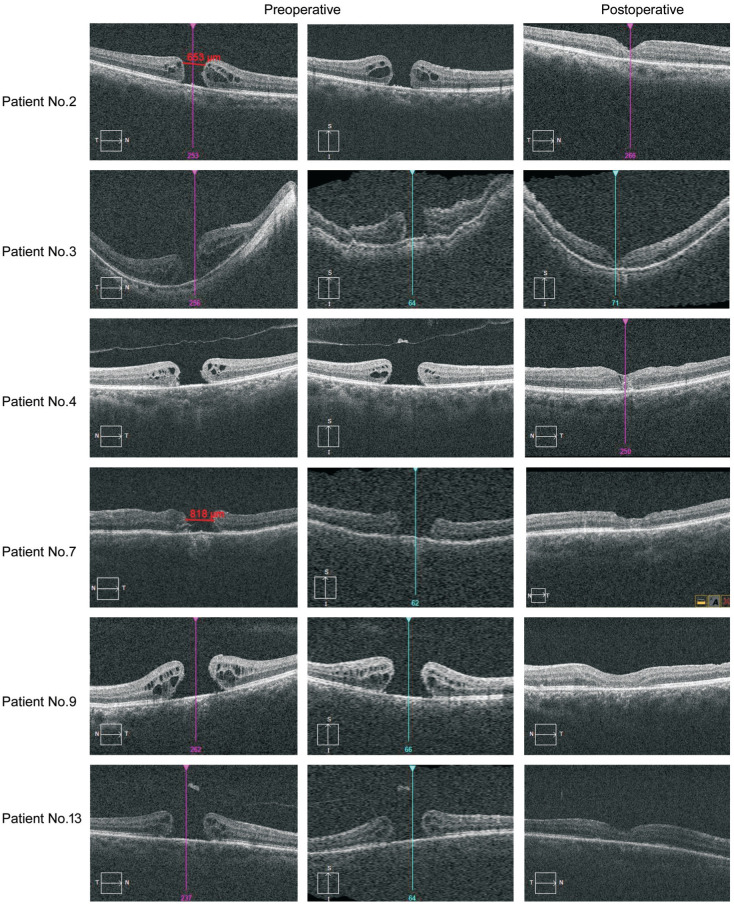
Methods: Patients with giant (minimum diameter ≥800 µm), recurrent or persistent MHs who underwent PPV combined with parafoveal retinal massage and autologous whole blood cover using C3F8 as tamponade agent from February 2018 to May 2019 were enrolled in this retrospective study. After surgery, all patients were informed to maintain a prone position for at least 7d. Preoperative and postoperative best-corrected visual acuities (BCVAs) were compared and MH closure rate was measured as the main outcome.
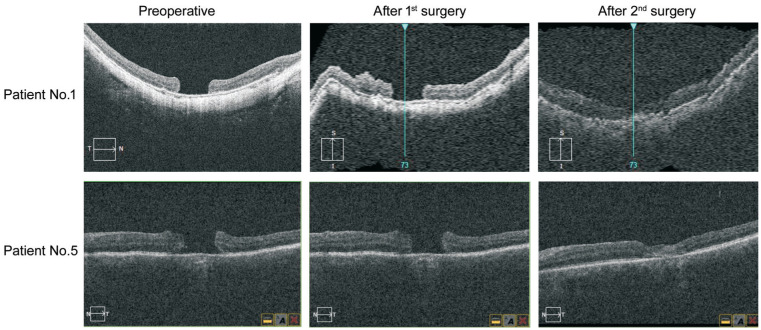
Results: A total of 13 MH patients consisted of 6 giant MHs, 4 persistent holes and 3 recurrent holes (5 men and 8 women; average age was 56.40±11.72y) were enrolled in this study. MH closure was achieved in 11 eyes by this modified surgical technique while 2 eyes failed. Revitrectomy with autologous neurosensory retinal patch transplantations was applied for those 2 patients and then both holes were closed. No intraoperative complications were observed. BCVA improved from 1.73 logMAR to 0.74 logMAR at 6mo postoperation. There was significant difference in BCVA before versus after the surgery (P<0.05). There were no adverse events occurred during the follow-up period.
Conclusion: With easier surgical procedure, parafoveal retinal massage combined with autologous whole blood cover is an effective addition to the surgical options for the management of refractory MHs.
Keywords: autologous blood cover; giant macular hole; parafoveal retinal massage; persistent macular hole; recurrent macular hole; vitrectomy.
International Journal of Ophthalmology Press.
Figures
References
-
- Oh H. Idiopathic macular hole. Dev Ophthalmol. 2014;54:150–158. - PubMed
-
- Grewal DS, Mahmoud TH, Fine HF. Management of challenging macular holes: current concepts and new surgical techniques. Ophthalmic Surg Lasers Imaging Retina. 2016;47(6):508–513. - PubMed
-
- Lee SM, Kwon HJ, Park SW, Lee JE, Byon IS. Microstructural changes in the fovea following autologous internal limiting membrane transplantation surgery for large macular holes. Acta Ophthalmol. 2018;96(3):e406–e408. - PubMed
LinkOut - more resources
Full Text Sources