

Human Immunodeficiency Virus-Infected Immunological Nonresponders Have Colon-Restricted Gut Mucosal Immune Dysfunction
- PMID: 33216130
- PMCID: PMC8844596
- DOI: 10.1093/infdis/jiaa714
Human Immunodeficiency Virus-Infected Immunological Nonresponders Have Colon-Restricted Gut Mucosal Immune Dysfunction
Abstract
Background: Human immunodeficiency virus (HIV)-infected immunological nonresponders (INRs) fail to reconstitute their CD4+ T-cell pool after initiation of antiretroviral therapy, and their prognosis is inferior to that of immunological responders (IRs). A prevailing hypothesis is that the INR phenotype is caused by a persistently disrupted mucosal barrier, but assessments of gut mucosal immunology in different anatomical compartments are scarce.
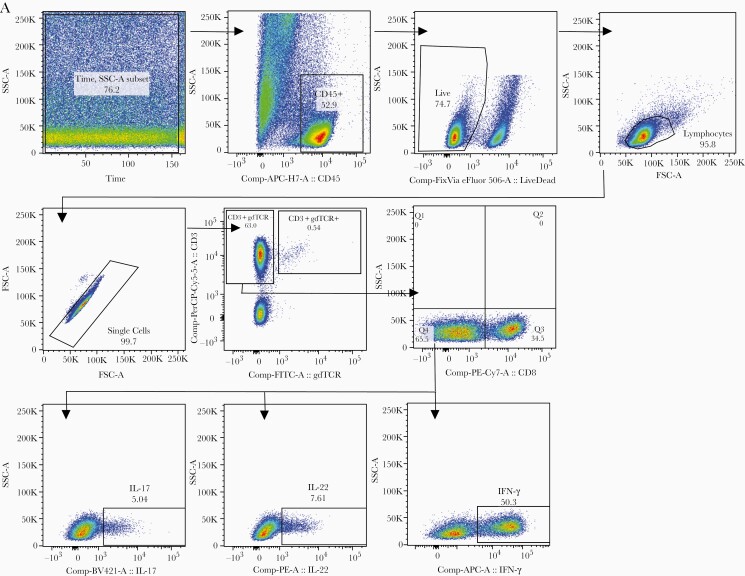
Methods: We investigated circulating markers of mucosal dysfunction, immune activation, mucosal Th17 and Th22 cells, and mucosa-adherent microbiota signatures in gut mucosal specimens from sigmoid colon and terminal ileum of 19 INRs and 20 IRs in addition to 20 HIV-negative individuals.
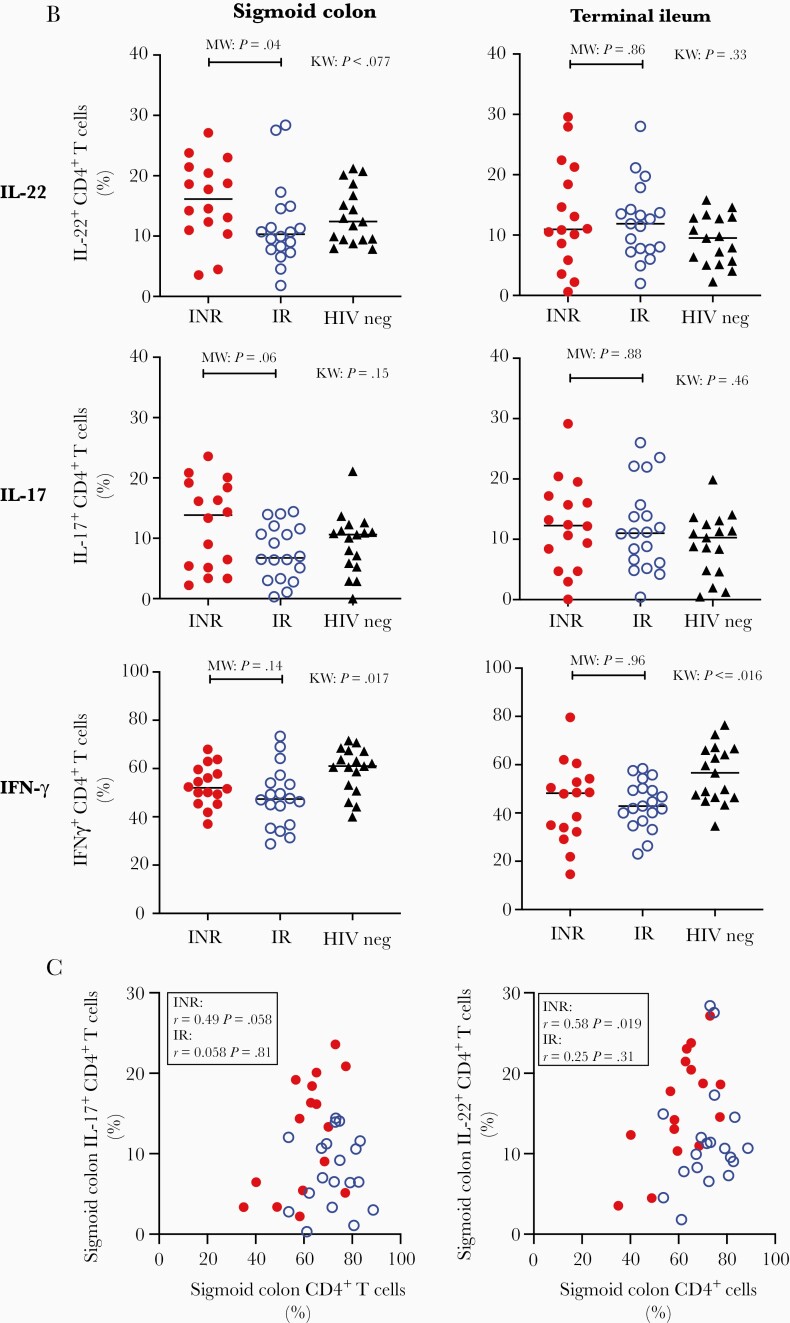
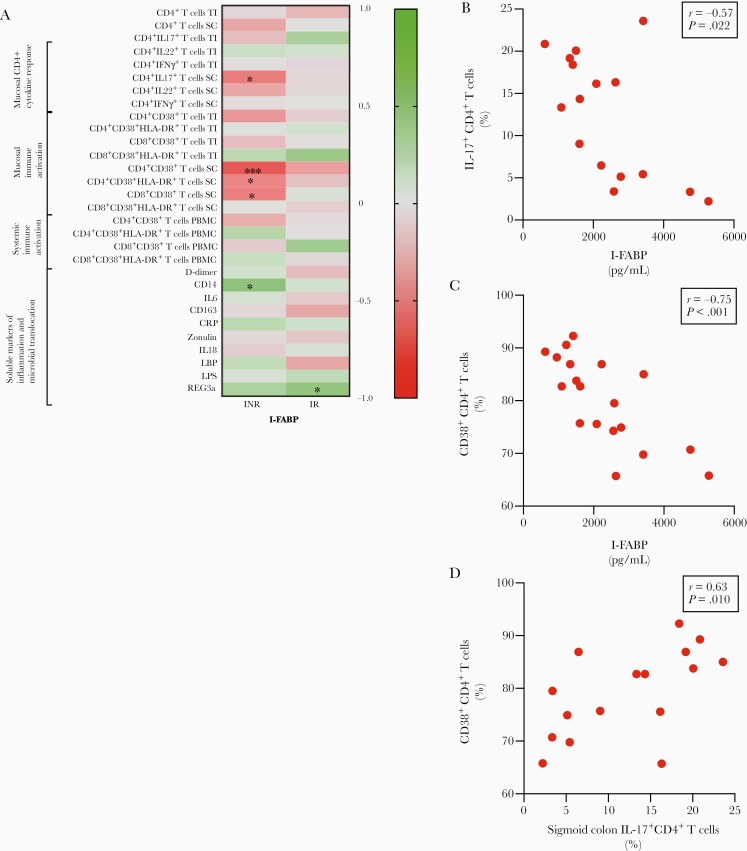
Results: INRs had higher blood levels of the enterocyte damage marker intestinal fatty acid-binding protein than IRs. In gut mucosal biopsies, INRs had lower fractions of CD4+ T cells, higher fractions of interleukin 22, and a tendency to higher fractions of interleukin 17-producing CD4+ T cells. These findings were all restricted to the colon and correlated to circulating markers of enterocyte damage. There were no observed differences in gut microbial composition between INRs and IRs.
Conclusions: Restricted to the colon, enterocyte damage and mucosal immune dysfunction play a role for insufficient immune reconstitution in HIV infection independent of the gut microbiota.
Keywords: HIV; gut microbiota; immunological nonresponders; mucosal immunology.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures




References
-
- Kim CJ, Nazli A, Rojas OL, et al. A role for mucosal IL-22 production and Th22 cells in HIV-associated mucosal immunopathogenesis. Mucosal Immunol 2012; 5:670–80. - PubMed
-
- Brenchley JM, Price DA, Schacker TW, et al. Microbial translocation is a cause of systemic immune activation in chronic HIV infection. Nat Med 2006; 12:1365–71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
