

Guiding Nipple-Areola Complex Reconstruction: Literature Review and Proposal of a New Decision-Making Algorithm
- PMID: 33216178
- PMCID: PMC8144123
- DOI: 10.1007/s00266-020-02047-9
Guiding Nipple-Areola Complex Reconstruction: Literature Review and Proposal of a New Decision-Making Algorithm
Abstract
Background: Nipple-areola complex reconstruction (NAR) most commonly represents the finishing touch to breast reconstruction (BR). Nipple presence is particularly relevant to the patient's psyche, beyond any shadow of doubt. Many reconstructive options have been described in time. Surgery is easy, but final result is often disappointing on the long run.
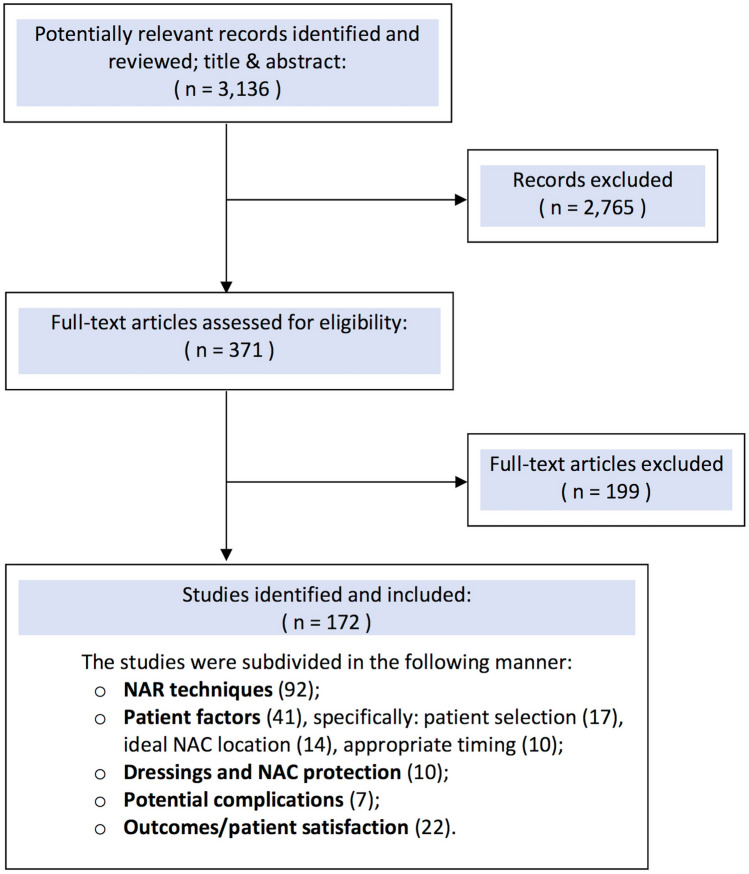
Methods: The goal of this manuscript is to analyze and classify knowledge concerning NAR techniques and the factors that influence success, and then to elaborate a practical evidence-based algorithm. Out of the 3136 available articles as of August 8th, 2020, we selected 172 manuscripts that met inclusion criteria, which we subdivided into 5 main topics of discussion, being the various NAR techniques; patient factors (including patient selection, timing and ideal position); dressings; potential complications and finally, outcomes/patient satisfaction.
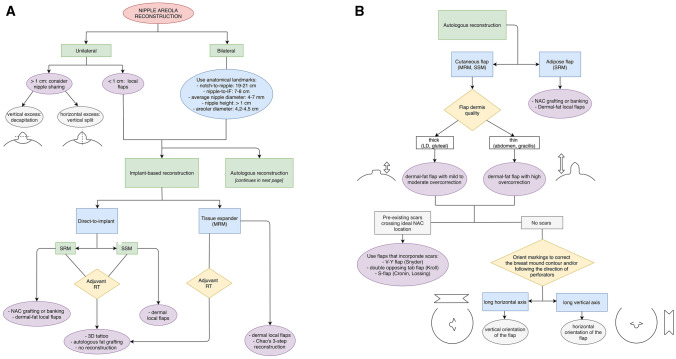
Results: We found 92 articles describing NAR techniques, 41 addressing patient factors (out of which 17 discussed patient selection, 14 described ideal NAC location, 10 described appropriate timing), 10 comparing dressings, 7 studying NAR complications, and 22 addressing outcomes and patient satisfaction. We elaborated a comprehensive decision-making algorithm to help narrow down the choice among NAR techniques, and choose the correct strategy according to the various scenarios, and particularly the BR technique and skin envelope.
Conclusions: No single NAR technique provides definitive results, which is why we believe there is no "end-all be-all solution". NAR must be approached as a case-by-case situation. Furthermore, despite NAR being such a widely discussed topic in scientific literature, we still found a lack of clinical trials to allow for more thorough recommendations to be elaborated.
Level of evidence iii: This journal requires that authors assign a level of evidence to each submission to which Evidence-Based Medicine rankings are applicable. This excludes Review Articles, Book Reviews, and manuscripts that concern Basic Science, Animal Studies, Cadaver Studies, and Experimental Studies. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Keywords: Breast cancer; Breast reconstruction; Nipple-areola complex; Nipple-areola reconstruction; Nipple-areola surgery.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures



Comment in
-
Invited Discussion on: Guiding Nipple-Areola Complex Reconstruction: Literature Review and Proposal of a New Decision-Making Algorithm.Aesthetic Plast Surg. 2021 Jun;45(3):946-947. doi: 10.1007/s00266-020-02076-4. Epub 2021 Jan 5. Aesthetic Plast Surg. 2021. PMID: 33403408 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
