

Closed-Loop Insulin Therapy Improves Glycemic Control in Adolescents and Young Adults: Outcomes from the International Diabetes Closed-Loop Trial
- PMID: 33216667
- PMCID: PMC8080922
- DOI: 10.1089/dia.2020.0572
Closed-Loop Insulin Therapy Improves Glycemic Control in Adolescents and Young Adults: Outcomes from the International Diabetes Closed-Loop Trial
Abstract
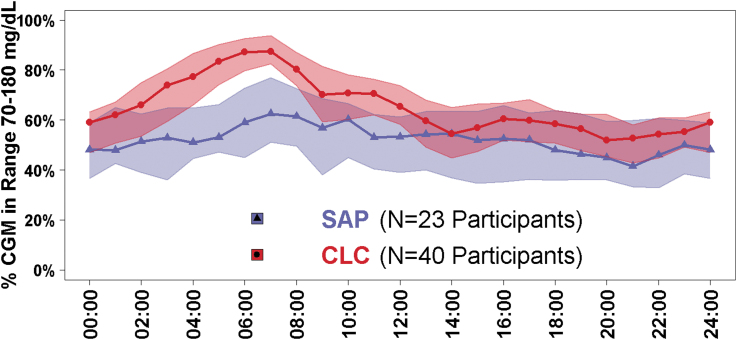
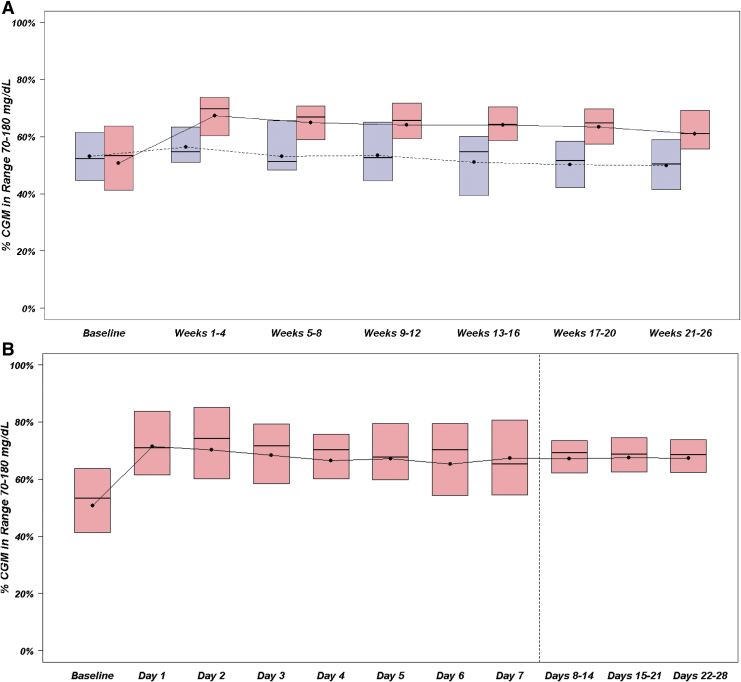
Objective: To assess the efficacy and safety of closed-loop control (CLC) insulin delivery system in adolescents and young adults with type 1 diabetes. Research Design and Methods: Prespecified subanalysis of outcomes in adolescents and young adults aged 14-24 years old with type 1 diabetes in a previously published 6-month multicenter randomized trial. Participants were randomly assigned 2:1 to CLC (Tandem Control-IQ) or sensor augmented pump (SAP, various pumps+Dexcom G6 CGM) and followed for 6 months. Results: Mean age of the 63 participants was 17 years, median type 1 diabetes duration was 7 years, and mean baseline HbA1c was 8.1%. All 63 completed the trial. Time in range (TIR) increased by 13% with CLC versus decreasing by 1% with SAP (adjusted treatment group difference = +13% [+3.1 h/day]; 95% confidence interval [CI] 9-16, P < 0.001), which largely reflected a reduction in time >180 mg/dL (adjusted difference -12% [-2.9 h/day], P < 0.001). Time <70 mg/dL decreased by 1.6% with CLC versus 0.3% with SAP (adjusted difference -0.7% [-10 min/day], 95% CI -1.0% to -0.2%, P = 0.002). CLC use averaged 89% of the time for 6 months. The mean adjusted difference in HbA1c after 6 months was 0.30% in CLC versus SAP (95% CI -0.67 to +0.08, P = 0.13). There was one diabetic ketoacidosis episode in the CLC group. Conclusions: CLC use for 6 months was substantial and associated with improved TIR and reduced hypoglycemia in adolescents and young adults with type 1 diabetes. Thus, CLC has the potential to improve glycemic outcomes in this challenging age group. The clinical trial was registered with ClinicalTrials.gov (NCT03563313).
Keywords: Adolescents; Closed-loop control insulin delivery; Time in range; Young adult.
Conflict of interest statement
D.R. has no disclosures to report. L.A.-O. has received consulting fees from Dexcom. J.E.P. reports receiving grant support, provided to his institution, consulting fees, and speaker fees from Tandem Diabetes Care, grant support, provided to his institution, and advisory board fees from Medtronic, grant support, provided to his institution, and consulting fees from Eli Lilly, grant support and supplies, provided to his institution, from Insulet, and supplies, provided to his institution, from Dexcom. B.A.B. has received research funding from Tandem, Insulet Corp., Medtronic, Beta Bionics, Lilly, Convatec, and Dexcom. He has served on advisory boards for Medtronic, Novo Nordisk, and Convatec. R.P.W. reports receiving grant support and supplies, provided to his institution, from Tandem Diabetes Care, Dexcom, Beta Bionics, Eli Lilly, and MannKind and has served as a consultant/speaker for Eli Lilly and Tandem Diabetes Care. L.E. serves as a consultant for Tandem Diabetes Care. Y.C.K. received product support from Dexcom and Roche Diabetes and has consulted for Novo Nordisk. C.J.L. reports receiving advisory board fees from Sanofi, and grant support, paid to her institution, from Dexcom, Tandem Diabetes Care, Insulet, Abbott Diabetes, Senseonics, and Lexicon Pharmaceuticals. G.P.F. conducts research supported by Medtronic, Dexcom, Abbott, Tandem, Insulet, Beta Bionics, and Lilly and has been a consultant/speaker for Medtronic, Dexcom, Abbott, Tandem, Insulet, Beta Bionics, and Lilly. R.W.B. reports receiving consulting fees, paid to his institution, from Insulet, Bigfoot Biomedical, vTv Therapeutics, and Eli Lilly, grant support and supplies, provided to his institution, from Tandem and Dexcom, and supplies from Ascenia and Roche. C.K. has received consulting fees, paid to his institution, from Bigfoot Biomedical and grant support and supplies, provided to his institution, from Tandem and Dexcom. J.W.L. reports receiving consulting fees, paid to his institution, from Animas Corporation, Bigfoot Biomedical, Tandem Diabetes Care, and Eli Lilly. S.A.B. reports receiving grant support and supplies, provided to her institution, from Tandem Diabetes Care, Insulet, and Tolerion, and supplies, provided to her institution, from Dexcom and Roche Diagnostics. L.M.L. has received consulting fees from Johnson & Johnson, Sanofi, NovoNordisk, Roche, Dexcom, Insulet, Boehringer Ingelheim, ConvaTec, Medtronic, Lifescan, Laxmi, and Insulogic.
Figures
References
-
- American Diabetes Association: 13. Children and adolescents: standards of medical care in diabetes-2020. Diabetes Care 2020;43:S163–S182 - PubMed
-
- Hermann JM, Miller KM, Hofer SE, et al. : The transatlantic HbA1c gap; differences in glycaemic control across the lifespan between people included in the US T1D Exchange Registry and those included in the German/Austrian DPV registry. Diabet Med 2020;37:848–855 - PubMed
-
- Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study Research Group: Mortality in type 1 diabetes in the DCCT/EDIC versus the general population. Diabetes Care 2016;39:1378–1383
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
