

The global burden of illness of peanut allergy: A comprehensive literature review
- PMID: 33216994
- PMCID: PMC8247890
- DOI: 10.1111/all.14666
The global burden of illness of peanut allergy: A comprehensive literature review
Abstract
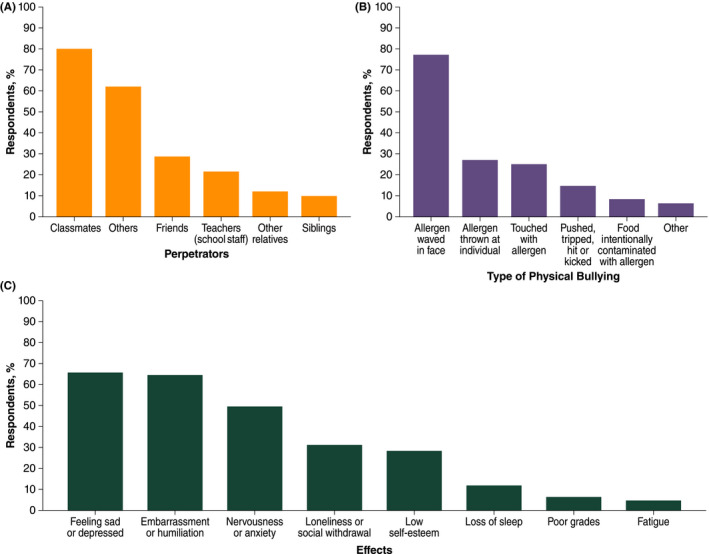
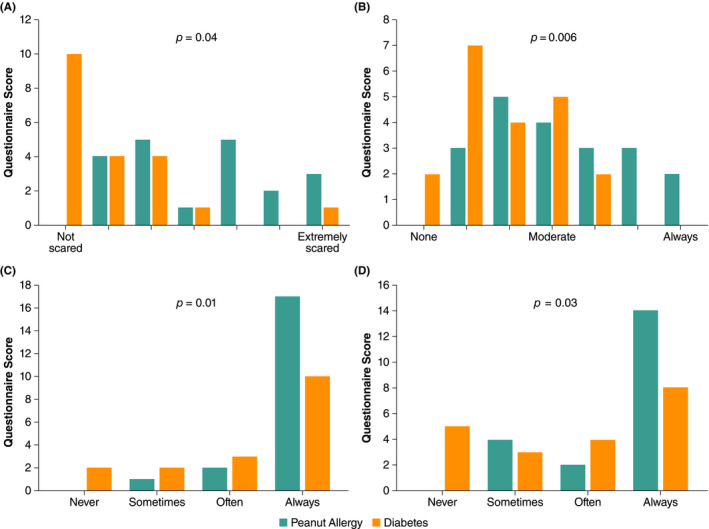
Peanut allergy (PA) currently affects approximately 2% of the general population of Western nations and may be increasing in prevalence. Patients with PA and their families/caregivers bear a considerable burden of self-management to avoid accidental peanut exposure and to administer emergency medication (adrenaline) if needed. Compared with other food allergies, PA is associated with higher rates of accidental exposure, severe reactions and potentially fatal anaphylaxis. Approximately 7%-14% of patients with PA experience accidental peanut exposure annually, and one-third to one-half may experience anaphylaxis, although fatalities are rare. These risks impose considerably high healthcare utilization and economic costs for patients with PA and restrictions on daily activities. Measures to accommodate patients with PA are often inadequate, with inconsistent standards for food labelling and inadequate safety policies in public establishments such as restaurants and schools. Children with PA are often bullied, resulting in sadness, humiliation and anxiety. These factors cumulatively contribute to significantly reduced health-related quality of life for patients with PA and families/caregivers. Such factors also provide essential context for risk/benefit assessments of new PA therapies. This narrative review comprehensively assessed the various factors comprising the burden of PA.
Keywords: accidental exposure; anaphylaxis; burden; health-related quality of life; peanut allergy.
© 2020 The Authors. Allergy published by European Academy of Allergy and Clinical Immunology and John Wiley & Sons Ltd.
Conflict of interest statement
JAL reports receiving research funding from and serving as an advisor to Aimmune Therapeutics and serving as an advisor to DBV Technologies and Covis Pharma. RG reports receiving grants from the National Institutes of Health (NIH), Stanford University, and Aimmune Therapeutics; serving as a medical consultant/advisor for DBV technologies, Aimmune, Before Brands, Pfizer, Mylan and Kaleo, Inc,; and receiving grants from the NIH, Allergy and Asthma Network, Food Allergy Research & Education, Rho Inc, Northwestern University Clinical and Translational Sciences Institute, Thermo Fisher, United Health Group, Mylan and the National Confectioners Association. RK is a consultant for Aimmune Therapeutics. TH is a former consultant for Aimmune Therapeutics. ST is an employee of Aimmune Therapeutics. DPM is a member of the Board of Directors for the Canadian Society of Allergy and Clinical Immunology; serves on the Editorial Board of the Journal of Food Allergy. He has provided consultation and speaker services for Pfizer, ALK, Aimmune, Merck, Covis and Pediapharm and has been part of an advisory board for ALK, Pfizer and Bausch Health. GP has provided consultation and speaker services for Aimmune Therapeutics, Bausch and Lomb, Stallergenes, ALK‐Abello; serves as a medical consultant/advisor for Bausch and Lomb.
Figures
References
-
- Skolnick HS, Conover‐Walker MK, Koerner CB, Sampson HA, Burks W, Wood RA. The natural history of peanut allergy. J Allergy Clin Immunol. 2001;107(2):367‐374. - PubMed
-
- Venter C, Maslin K, Patil V, et al. The prevalence, natural history and time trends of peanut allergy over the first 10 years of life in two cohorts born in the same geographical location 12 years apart. Pediatr Allergy Immunol. 2016;27(8):804‐811. - PubMed
-
- Deschildre A, Elegbede CF, Just J, et al. Peanut‐allergic patients in the MIRABEL survey: characteristics, allergists' dietary advice and lessons from real life. Clin Exp Allergy. 2016;46(4):610‐620. - PubMed
-
- Vereda A, van Hage M, Ahlstedt S, et al. Peanut allergy: clinical and immunologic differences among patients from 3 different geographic regions. J Allergy Clin Immunol. 2011;127(3):603‐607. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
