

Comparison of infection risks and clinical outcomes in patients with and without SARS-CoV-2 lung infection under renin-angiotensin-aldosterone system blockade: Systematic review and meta-analysis
- PMID: 33217033
- PMCID: PMC7753617
- DOI: 10.1111/bcp.14660
Comparison of infection risks and clinical outcomes in patients with and without SARS-CoV-2 lung infection under renin-angiotensin-aldosterone system blockade: Systematic review and meta-analysis
Abstract
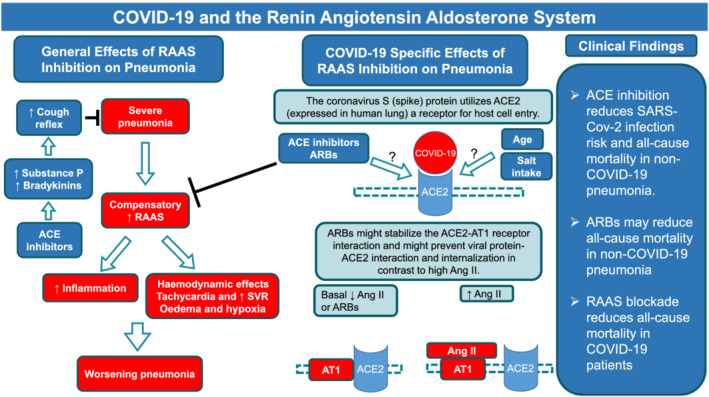
Aims: Angiotensin-converting enzyme-2 (ACE2) is the receptor for SARS-CoV-2. Animal studies suggest that renin-angiotensin-aldosterone system (RAAS) blockers might increase the expression of ACE2 and potentially increase the risk of SARS-CoV-2 infection.
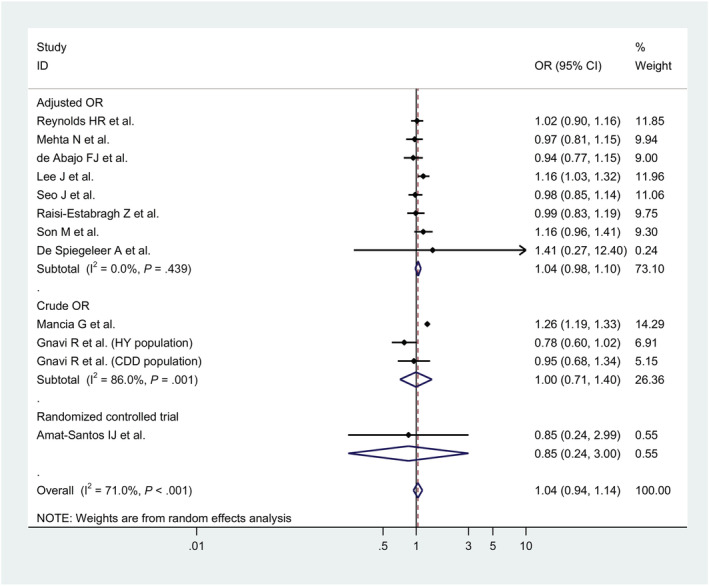
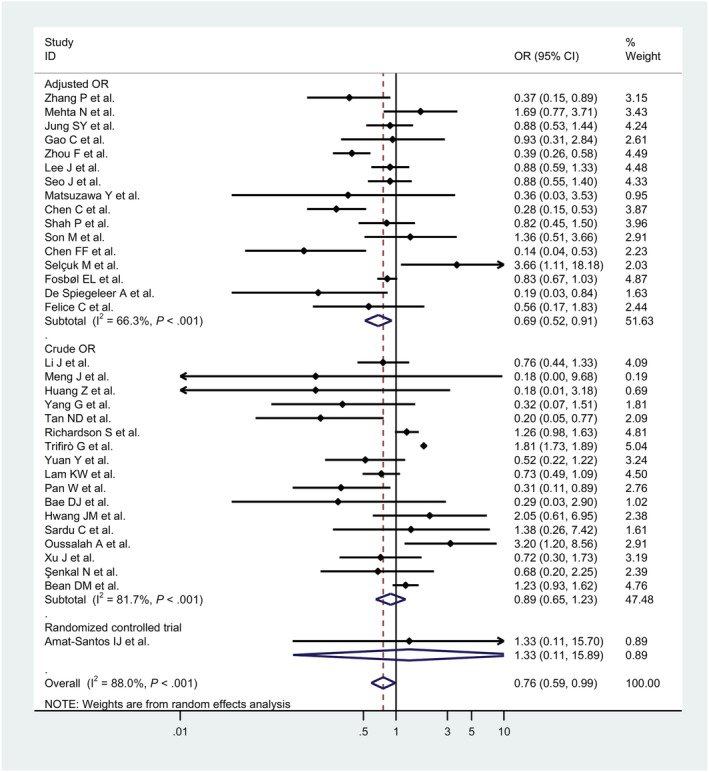
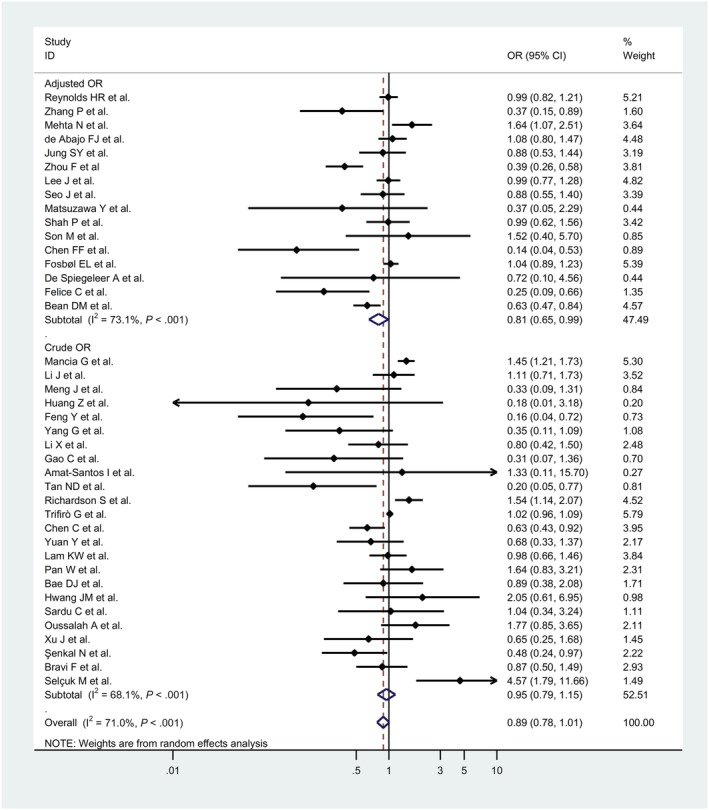
Methods and results: The effect of ACE inhibitor (ACEI) treatment on the pneumonia incidence in non-COVID-19 patients (25 studies, 330 780 patients) was associated with a 26% reduction of pneumonia risk (odds ratio [OR]: 0.74, P < .001). Pneumonia-related death cases in ACEI-treated non-COVID-19 patients were reduced by 27% (OR: 0.73, P = .004). However, angiotensin II receptor blockers (ARB) treatment (10 studies, 275 621 non-COVID-19 patients) did not alter pneumonia risk in patients. Pneumonia-related death cases in ARB-treated non-COVID-19 patients was analysed only in 1 study and was significantly reduced (OR, 0.47; 95% confidence interval, 0.30 to 0.72). Results from 11 studies (8.4 million patients) showed that the risk of getting infected with the SARS-CoV-2 virus was reduced by 13% (OR: 0.87, P = .014) in patients treated with ACEI, whereas analysis from 10 studies (8.4 million patients) treated with ARBs showed no effect (OR, 0.92, P = .354). Results from 34 studies in 67 644 COVID-19 patients showed that RAAS blockade reduces all-cause mortality by 24% (OR = 0.76, P = .04).
Conclusion: ACEIs reduce the risk of getting infected with the SARS-CoV-2 virus. Blocking the RAAS may decrease all-cause mortality in COVID-19 patients. ACEIs also reduce the risk of non-COVID pneumonia. All-cause mortality due to non-COVID pneumonia is reduced by ACEI and potentially by ARBs.
Keywords: ACE inhibitors; ACE2; SARS-CoV-2; angiotensin II receptor blockers.
© 2020 The Authors. British Journal of Clinical Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
RAAS Blockade and COVID-19: Mechanistic Modeling of Mas and AT1 Receptor Occupancy as Indicators of Pro-Inflammatory and Anti-Inflammatory Balance.Clin Pharmacol Ther. 2021 Apr;109(4):1092-1103. doi: 10.1002/cpt.2177. Epub 2021 Mar 10. Clin Pharmacol Ther. 2021. PMID: 33506503 Free PMC article.
-
SARS-CoV-2 and the Angiotensin-Converting Enzyme 2 Receptor: Angiotensin-Converting Enzyme Inhibitor/Angiotensin 2 Receptor Blocker Utilization and a Shift Towards the Renin-Angiotensin-Aldosterone System Classical Pathway.Cureus. 2024 Mar 5;16(3):e55563. doi: 10.7759/cureus.55563. eCollection 2024 Mar. Cureus. 2024. PMID: 38576704 Free PMC article. Review.
-
The use of renin-angiotensin-aldosterone system (RAAS) inhibitors is associated with a lower risk of mortality in hypertensive COVID-19 patients: A systematic review and meta-analysis.J Med Virol. 2021 Mar;93(3):1370-1377. doi: 10.1002/jmv.26625. Epub 2020 Nov 10. J Med Virol. 2021. PMID: 33095513
-
Effect of Renin-Angiotensin-Aldosterone System Inhibitors in Patients with COVID-19: a Systematic Review and Meta-analysis of 28,872 Patients.Curr Atheroscler Rep. 2020 Aug 24;22(10):61. doi: 10.1007/s11883-020-00880-6. Curr Atheroscler Rep. 2020. PMID: 32830286 Free PMC article.
-
Renin-angiotensin-aldosterone system inhibitors and SARS-CoV-2 infection: an analysis from the veteran's affairs healthcare system.Am Heart J. 2021 Oct;240:46-57. doi: 10.1016/j.ahj.2021.06.004. Epub 2021 Jun 12. Am Heart J. 2021. PMID: 34126079 Free PMC article.
Cited by
-
New perspectives on angiotensin-converting enzyme 2 and its related diseases.World J Diabetes. 2021 Jun 15;12(6):839-854. doi: 10.4239/wjd.v12.i6.839. World J Diabetes. 2021. PMID: 34168732 Free PMC article. Review.
-
Association of Finerenone Use With Reduction in Treatment-Emergent Pneumonia and COVID-19 Adverse Events Among Patients With Type 2 Diabetes and Chronic Kidney Disease: A FIDELITY Pooled Secondary Analysis.JAMA Netw Open. 2022 Oct 3;5(10):e2236123. doi: 10.1001/jamanetworkopen.2022.36123. JAMA Netw Open. 2022. PMID: 36287567 Free PMC article. Clinical Trial.
-
Safety of COVID-19 vaccination in women undergoing IVF/ICSI treatment - Clinical study and systematic review.Front Immunol. 2023 Jan 11;13:1054273. doi: 10.3389/fimmu.2022.1054273. eCollection 2022. Front Immunol. 2023. PMID: 36713439 Free PMC article.
-
Impact of hypertension on long-term humoral and cellular response to SARS-CoV-2 infection.Front Immunol. 2022 Sep 2;13:915001. doi: 10.3389/fimmu.2022.915001. eCollection 2022. Front Immunol. 2022. PMID: 36119050 Free PMC article.
-
Meta-analysis of the association between angiotensin pathway inhibitors and COVID-19 severity and mortality.Syst Rev. 2021 Sep 7;10(1):243. doi: 10.1186/s13643-021-01802-6. Syst Rev. 2021. PMID: 34488897 Free PMC article.
References
-
- Mortensen EM, Coley CM, Singer DE, et al. Causes of death for patients with community‐acquired pneumonia: results from the pneumonia patient outcomes research team cohort study. Arch Intern Med. 2002;162(9):1059‐1064. - PubMed
-
- Maclure M. The case‐crossover design: a method for studying transient effects on the risk of acute events. Am J Epidemiol. 2017;185(11):1174‐1183. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
