

Comparison of the intraoperative analgesic efficacy between ultrasound-guided deep and superficial serratus anterior plane block during video-assisted thoracoscopic lobectomy: A prospective randomized clinical trial
- PMID: 33217833
- PMCID: PMC7676537
- DOI: 10.1097/MD.0000000000023214
Comparison of the intraoperative analgesic efficacy between ultrasound-guided deep and superficial serratus anterior plane block during video-assisted thoracoscopic lobectomy: A prospective randomized clinical trial
Abstract
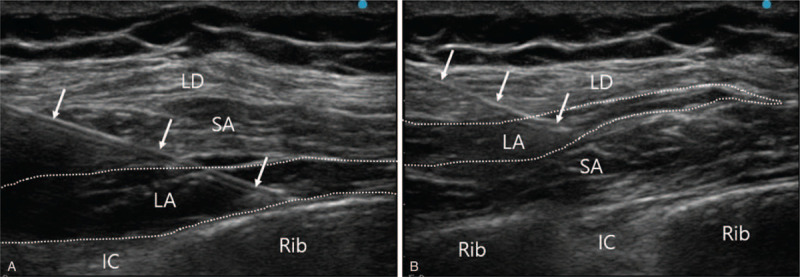
Background: The serratus anterior plane block (SAPB) is a novel method that provides lateral chest wall analgesia. There are 2 methods of SAPB; deep and superficial SAPB. Each of these methods has been demonstrated to provide effective perioperative analgesia in thoracic surgery. The aim of this study was to compare the intraoperative hemodynamic and analgesic benefits of deep versus superficial SAPB during video-assisted thoracic surgery (VATS) lobectomy.
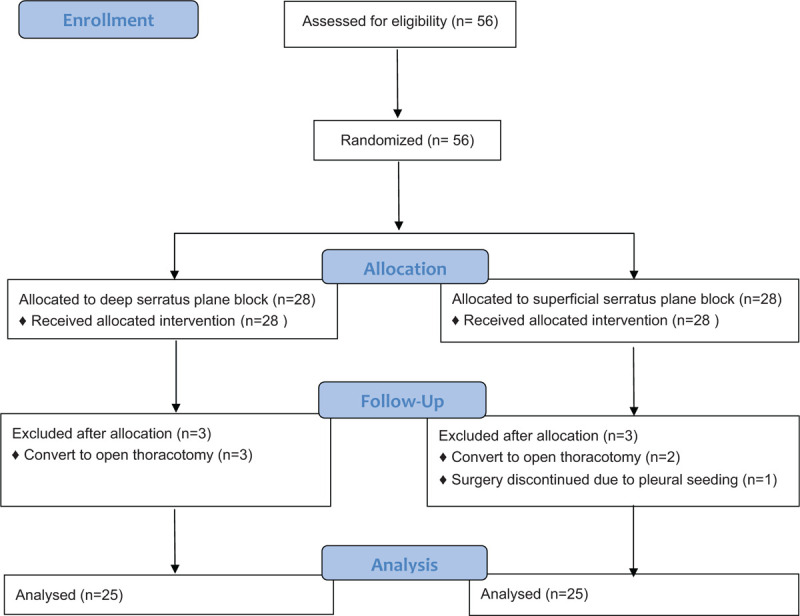
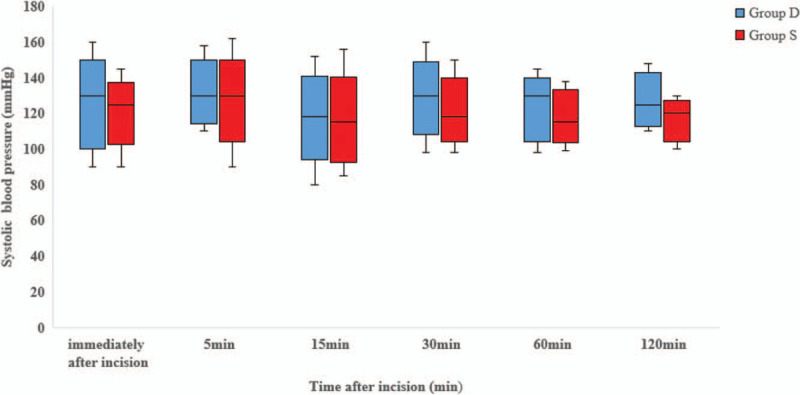
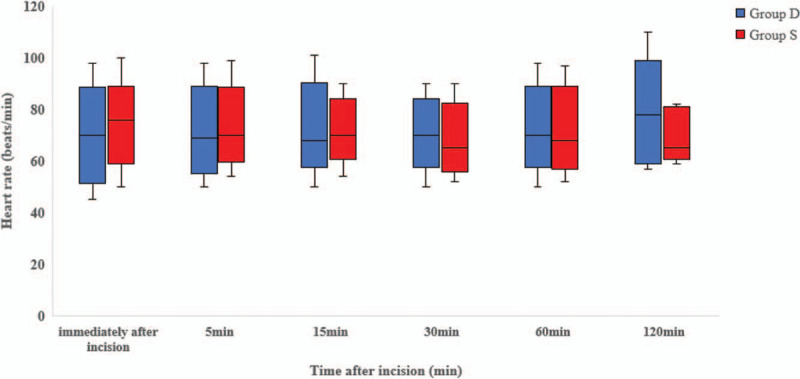
Methods: We performed a prospective, randomized, patient/assessor-blinded trial. We included patients who were 20 to 75 years of age and scheduled to undergo VATS lobectomy with American Society of Anesthesiologists physical status 1 or 2. Patients were randomly allocated to receive either ultrasound-guided deep SAPB (Group D) or superficial SAPB (Group S). The primary outcome was intraoperative remifentanil consumption. We also recorded intraoperative systolic blood pressure (SBP), heart rate (HR), emergence time, and doses of rescue drugs used to manage hemodynamic instability.
Results: Data for 50 patients undergoing 3-port VATS lobectomy were analyzed. Intraoperative remifentanil consumption did not differ significantly between Group D (n = 25, 715.62 ± 320.36 μg) and group S (n = 25, 721.08 ± 294.48 μg) (P = .97). Additionally, there were no significant differences between the 2 groups in SBP and HR at any time point, emergence time, or amount of rescue drugs used.
Conclusion: Our study suggests that the intraoperative analgesic efficacy is similar for deep and superficial SAPB during VATS lobectomy.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
The impact of hydromorphone combined with ropivacaine in serratus anterior plane block on postoperative pain in patients undergoing video-assisted thoracoscopic pulmonary lobectomy: a randomized, double-blind clinical trial.BMC Anesthesiol. 2025 May 10;25(1):237. doi: 10.1186/s12871-025-03101-2. BMC Anesthesiol. 2025. PMID: 40348971 Free PMC article. Clinical Trial.
-
The effects of ultrasound-guided serratus plane block, in combination with general anesthesia, on intraoperative opioid consumption, emergence time, and hemodynamic stability during video-assisted thoracoscopic lobectomy: A randomized prospective study.Medicine (Baltimore). 2019 May;98(18):e15385. doi: 10.1097/MD.0000000000015385. Medicine (Baltimore). 2019. PMID: 31045789 Free PMC article. Clinical Trial.
-
The Effect of Erector Spinae Plane Block and Combined Deep and Superficial Serratus Anterior Plane Block on Acute Pain After Video-Assisted Thoracoscopic Surgery: A Randomized Controlled Study.J Cardiothorac Vasc Anesth. 2022 Aug;36(8 Pt B):2991-2999. doi: 10.1053/j.jvca.2022.01.048. Epub 2022 Feb 4. J Cardiothorac Vasc Anesth. 2022. PMID: 35249833 Clinical Trial.
-
Analgesic Effectiveness of Perioperative Ultrasound-Guided Serratus Anterior Plane Block Combined with General Anesthesia in Patients Undergoing Video-Assisted Thoracoscopic Surgery: A Systematic Review and Meta-analysis.Pain Med. 2020 Oct 1;21(10):2412-2422. doi: 10.1093/pm/pnaa125. Pain Med. 2020. PMID: 32488265
-
Serratus Anterior Plane Block for Pain Management After Video-Assisted Thoracoscopic Surgeries: A Narrative Review.Medicina (Kaunas). 2025 May 28;61(6):1010. doi: 10.3390/medicina61061010. Medicina (Kaunas). 2025. PMID: 40572697 Free PMC article. Review.
Cited by
-
Analgesic effectiveness of serratus anterior plane block in patients undergoing video-assisted thoracoscopic surgery: a systematic review and updated meta-analysis of randomized controlled trials.BMC Anesthesiol. 2023 Jul 13;23(1):235. doi: 10.1186/s12871-023-02197-8. BMC Anesthesiol. 2023. PMID: 37442948 Free PMC article.
-
Ultrasound-guided deep versus superficial continuous serratus anterior plane block for pain management in patients with multiple rib fractures: A prospective randomized double-blind clinical trial.Saudi J Anaesth. 2025 Jan-Mar;19(1):58-64. doi: 10.4103/sja.sja_493_24. Epub 2025 Jan 1. Saudi J Anaesth. 2025. PMID: 39958314 Free PMC article.
-
Comparison of combined deep and superficial serratus anterior block with thoracic paravertebral block for postoperative pain in patients undergoing video-assisted thoracoscopic surgery.Turk J Med Sci. 2024 Aug 4;54(5):1021-1032. doi: 10.55730/1300-0144.5881. eCollection 2024. Turk J Med Sci. 2024. PMID: 39473759 Free PMC article.
-
Efficacy of Intrathoracic Intercostal Nerve Block on Postoperative Acute and Chronic Pains of Patients Undergoing Video-Assisted Thoracoscopic Surgery.J Pain Res. 2022 Aug 6;15:2273-2281. doi: 10.2147/JPR.S369042. eCollection 2022. J Pain Res. 2022. PMID: 35967470 Free PMC article. Clinical Trial.
-
Analgesic efficacy and safety of erector spinae plane block versus serratus anterior plane block in breast surgery-a meta-analysis and systematic review of randomized controlled trials.J Anesth Analg Crit Care. 2024 Dec 18;4(1):82. doi: 10.1186/s44158-024-00218-7. J Anesth Analg Crit Care. 2024. PMID: 39695870 Free PMC article. Review.
References
-
- Ochroch EA, Gottschalk A. Impact of acute pain and its management for thoracic surgical patients. Thorac Surg Clin 2005;15:105–21. - PubMed
-
- Ochroch EA, Gottschalk A, Augostides J, et al. Long-term pain and activity during recovery from major thoracotomy using thoracic epidural analgesia. Anesthesiology 2002;97:1234–44. - PubMed
-
- Rogers ML, Henderson L, Mahajan RP, et al. Preliminary findings in the neurophysiological assessment of intercostal nerve injury during thoracotomy. Eur J Cardiothorac Surg 2002;21:298–301. - PubMed
-
- Pintaric TS, Potocnik I, Hadzic A, et al. Comparison of continuous thoracic epidural with paravertebral block on perioperative analgesia and hemodynamic stability in patients having open lung surgery. Reg Anesth Pain Med 2011;36:256–60. - PubMed
-
- Kaplowitz J, Papadakos PJ. Acute pain management for video-assisted thoracoscopic surgery: an update. J Cardiothorac Vasc Anesth 2012;26:312–21. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
