

Simultaneous renal clear cell carcinoma and primary clear cell carcinoma of the liver: A case report
- PMID: 33217850
- PMCID: PMC7676612
- DOI: 10.1097/MD.0000000000023263
Simultaneous renal clear cell carcinoma and primary clear cell carcinoma of the liver: A case report
Abstract
Rationale: Double primary clear cell carcinomas of the liver (PCCCL) and kidney are extremely rare; moreover, there have been no reported cases of adrenal metastasis from primary clear cell tumors of the liver.
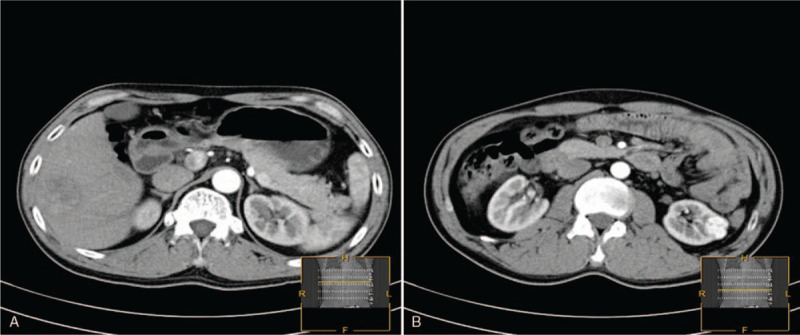
Patient concerns: A 47-year-old male patient was admitted to our clinic with space-occupying lesions in the left kidney and liver during a regular medical examination.
Diagnoses: The tumors in the kidney and liver were diagnosed as primary clear cell carcinoma by histopathological examination.
Interventions: The patient subsequently underwent nephron-sparing surgery of the left kidney and radical partial excision of the right liver lobe by laparoscopic surgery. Transcatheter arterial chemoembolization (TACE) was performed for the patient 2 weeks after tumor resection. One month after the operation, the patient started adjuvant therapy with sorafenib (400 mg twice per day orally). However, follow-up CT imaging revealed a solid mass measuring 1.9 × 2.0 × 2.0 cm in the right adrenal gland at 2 months postoperatively, and then the patient underwent radiofrequency ablation (RFA) for the right adrenal tumor.
Outcomes: The patient remained cancer free for 2 years following the diagnosis despite early right adrenal metastasis.
Lessons: Hepatocyte immunostaining is sufficient for the diagnosis of PCCCL.
Conflict of interest statement
The authors have no funding and conflicts of interests to disclose.
Figures



Similar articles
-
Simultaneous double primary clear cell carcinomas of liver and kidney: a case report and review of literature.Int J Clin Exp Pathol. 2015 Jan 1;8(1):995-9. eCollection 2015. Int J Clin Exp Pathol. 2015. PMID: 25755808 Free PMC article. Review.
-
[Bilateral kidney tumor. Therapy management and histopathological results with long-term follow-up of 66 patients].Urologe A. 2001 Mar;40(2):114-20. doi: 10.1007/s001200050448. Urologe A. 2001. PMID: 11315585 German.
-
Histopathologic confirmation of complete cancer-cell kill in excised specimens after renal cryotherapy.Urology. 2004 Sep;64(3):590. doi: 10.1016/j.urology.2004.05.010. Urology. 2004. PMID: 15351611
-
Retroperitoneal and intrahepatic metastasis from primary clear cell carcinoma of the liver: A case report and review of the literature.Medicine (Baltimore). 2017 Mar;96(12):e6452. doi: 10.1097/MD.0000000000006452. Medicine (Baltimore). 2017. PMID: 28328858 Free PMC article.
-
Renal hybrid oncocytic/chromophobe tumor associated with multiple schwannomas: Case report and literature review.Medicine (Baltimore). 2017 Dec;96(48):e8939. doi: 10.1097/MD.0000000000008939. Medicine (Baltimore). 2017. PMID: 29310387 Free PMC article. Review.
Cited by
-
Diagnosis of primary clear cell carcinoma of the liver based on Faster region-based convolutional neural network.Chin Med J (Engl). 2023 Nov 20;136(22):2706-2711. doi: 10.1097/CM9.0000000000002853. Epub 2023 Oct 25. Chin Med J (Engl). 2023. PMID: 37882066 Free PMC article. Clinical Trial.
-
Primary Synchronous Ipsilateral Renal Fibrosarcoma and Renal Pelvic Carcinoma: A Case Report and Literature Review.Onco Targets Ther. 2021 Jul 7;14:4119-4125. doi: 10.2147/OTT.S317094. eCollection 2021. Onco Targets Ther. 2021. PMID: 34262296 Free PMC article.
-
Hepatocellular carcinoma complicated with huge posterior pancreas head lymph node metastasis and primary renal carcinoma: A case report.Front Oncol. 2022 Dec 8;12:989172. doi: 10.3389/fonc.2022.989172. eCollection 2022. Front Oncol. 2022. PMID: 36568158 Free PMC article.
References
-
- Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 2016;27: suppl 5: 58–68. - PubMed
-
- Demandante CG, Troyer DA, Miles TP. Multiple primary malignant neoplasms: case report and a comprehensive review of the literature. Am J Clin Oncol 2003;26:79–83. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
