

Household presentation of influenza and acute respiratory illnesses to a primary care sentinel network: retrospective database studies (2013-2018)
- PMID: 33218318
- PMCID: PMC7677442
- DOI: 10.1186/s12889-020-09790-3
Household presentation of influenza and acute respiratory illnesses to a primary care sentinel network: retrospective database studies (2013-2018)
Abstract
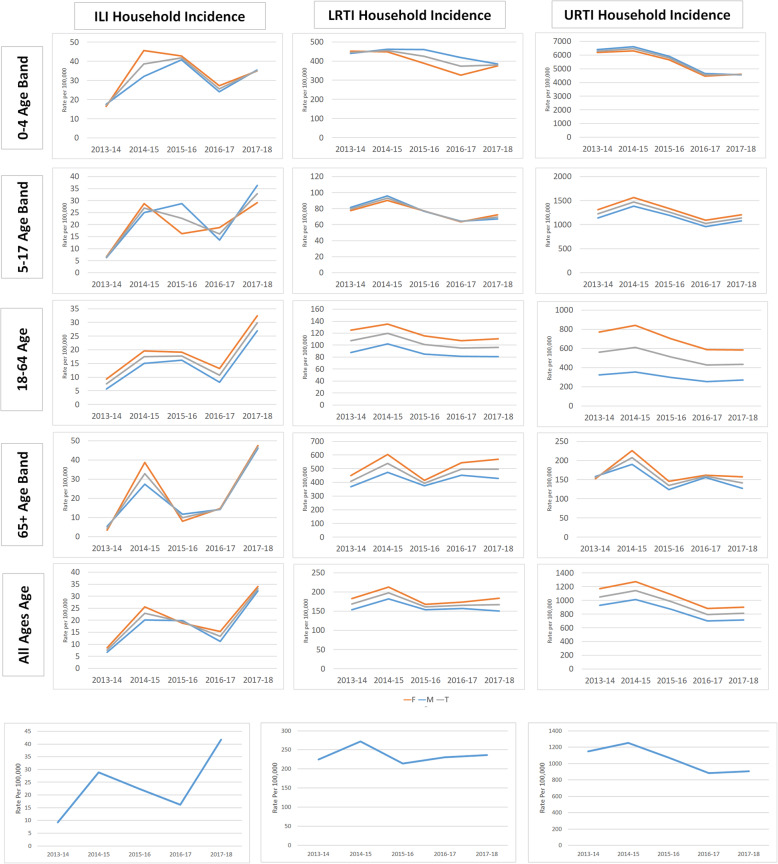
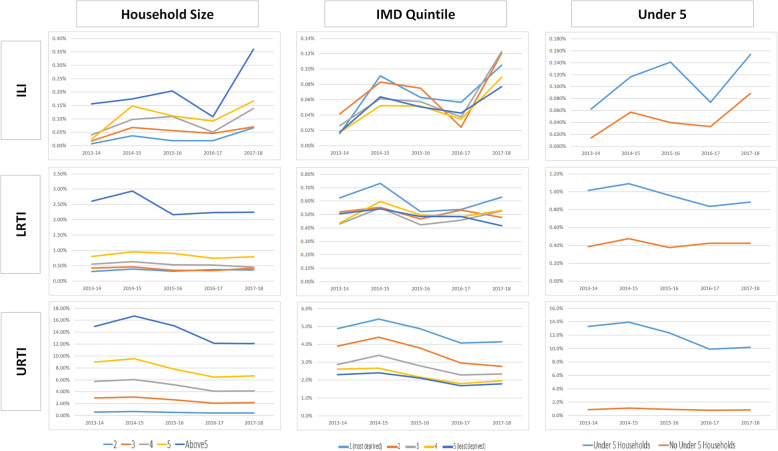
Background: Direct observation of the household spread of influenza and respiratory infections is limited; much of our understanding comes from mathematical models. The study aims to determine household incidence of influenza-like illness (ILI), lower (LRTI) and upper (URTI) respiratory infections within a primary care routine data and identify factors associated with the diseases' incidence.
Methods: We conducted two five-year retrospective analyses of influenza-like illness (ILI), lower (LRTI) and upper (URTI) respiratory infections using the England Royal College of General Practitioners (RCGP) Research and Surveillance Centre (RSC) primary care sentinel network database; a cross-sectional study reporting incident rate ratio (IRR) from a negative binomial model and a retrospective cohort study, using a shared gamma frailty survival model, reporting hazard ratios (HR). We reported the following household characteristics: children < 5 years old, each extra household member, gender, ethnicity (reference white), chronic disease, pregnancy, and rurality.
Results: The IRR where there was a child < 5 years were 1·62 (1·38-1·89, p < 0·0001), 2·40 (2.04-2.83, p < 0·0001) and 4·46 (3.79-5.255, p < 0·0001) for ILI, LRTI and URTI respectively. IRR also increased with household size, rurality and presentations and by female gender, compared to male. Household incidence of URTI and LRTI changed little between years whereas influenza did and were greater in years with lower vaccine effectiveness. The HR where there was a child < 5 years were 2·34 (95%CI 1·88-2·90, p < 0·0001), 2·97 (95%CI 2·76-3·2, p < 0·0001) and 10·32 (95%CI 10.04-10.62, p < 0·0001) for ILI, LRTI and URTI respectively. HR were increased with female gender, rurality, and increasing household size.
Conclusions: Patterns of household incidence can be measured from routine data and may provide insights for the modelling of disease transmission and public health policy.
Keywords: Computerized; Disease incidence; Family characteristics; Infectious; Medical record systems; Population characteristics.
Conflict of interest statement
SdeL is the Director of RCGP RSC, principally funded by PHE. He has received funding from GSK and Seqirus through the University of Surrey to study the monitoring of vaccine adverse events and attitudes to flu vaccination, respectively. He has attended advisory Boards for Sanofi and Seqirus.
Figures
Similar articles
-
Postpandemic Sentinel Surveillance of Respiratory Diseases in the Context of the World Health Organization Mosaic Framework: Protocol for a Development and Evaluation Study Involving the English Primary Care Network 2023-2024.JMIR Public Health Surveill. 2024 Apr 3;10:e52047. doi: 10.2196/52047. JMIR Public Health Surveill. 2024. PMID: 38569175 Free PMC article.
-
Household presentation of acute gastroenteritis in a primary care sentinel network: retrospective database studies.BMC Public Health. 2020 Apr 5;20(1):445. doi: 10.1186/s12889-020-08525-8. BMC Public Health. 2020. PMID: 32248812 Free PMC article.
-
Incidence of household transmission of acute gastroenteritis (AGE) in a primary care sentinel network (1992-2017): cross-sectional and retrospective cohort study protocol.BMJ Open. 2018 Aug 23;8(8):e022524. doi: 10.1136/bmjopen-2018-022524. BMJ Open. 2018. PMID: 30139907 Free PMC article.
-
PRINCIPLE trial demonstrates scope for in-pandemic improvement in primary care antibiotic stewardship: a retrospective sentinel network cohort study.BJGP Open. 2021 Oct 26;5(5):BJGPO.2021.0087. doi: 10.3399/BJGPO.2021.0087. Print 2021 Oct. BJGP Open. 2021. PMID: 34312163 Free PMC article.
-
Do influenza and acute respiratory infective diseases weigh heavily on general practitioners' daily practice?Eur J Gen Pract. 2006;12(1):34-6. doi: 10.1080/13814780600757153. Eur J Gen Pract. 2006. PMID: 16945870
Cited by
-
Responding to COVID-19 with real-time general practice data in Australia.Int J Med Inform. 2022 Jan;157:104624. doi: 10.1016/j.ijmedinf.2021.104624. Epub 2021 Oct 29. Int J Med Inform. 2022. PMID: 34741891 Free PMC article.
-
Investigating the uptake, effectiveness and safety of COVID-19 vaccines: protocol for an observational study using linked UK national data.BMJ Open. 2022 Feb 14;12(2):e050062. doi: 10.1136/bmjopen-2021-050062. BMJ Open. 2022. PMID: 35165107 Free PMC article.
-
Postpandemic Sentinel Surveillance of Respiratory Diseases in the Context of the World Health Organization Mosaic Framework: Protocol for a Development and Evaluation Study Involving the English Primary Care Network 2023-2024.JMIR Public Health Surveill. 2024 Apr 3;10:e52047. doi: 10.2196/52047. JMIR Public Health Surveill. 2024. PMID: 38569175 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
