

Clinical features which predict neuronal surface autoantibodies in new-onset focal epilepsy: implications for immunotherapies
- PMID: 33219046
- PMCID: PMC7892387
- DOI: 10.1136/jnnp-2020-325011
Clinical features which predict neuronal surface autoantibodies in new-onset focal epilepsy: implications for immunotherapies
Abstract
Objective: To generate a score which clinically identifies surface-directed autoantibodies in adults with new-onset focal epilepsy, and evaluate the value of immunotherapy in this clinical setting.
Methods: Prospective clinical and autoantibody evaluations in a cohort of 219 consecutive patients with new-onset focal epilepsy.
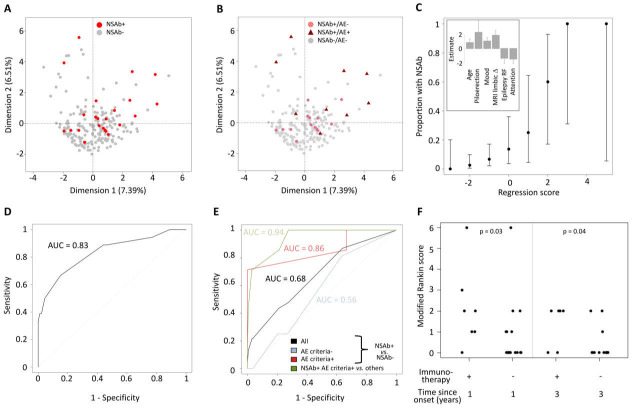
Results: 10.5% (23/219) of people with new-onset focal epilepsy had detectable serum autoantibodies to known or novel cell surface antigenic targets. 9/23 with autoantibodies were diagnosed with encephalitis, by contrast to 0/196 without autoantibodies (p<0.0001). Multivariate analysis identified six features which predicted autoantibody positivity (area under the curve=0.83): age ≥54 years, ictal piloerection, lowered self-reported mood, reduced attention, MRI limbic system changes and the absence of conventional epilepsy risk factors. 11/14 (79%) patients with detectable autoantibodies, but without encephalitis, showed excellent long-term outcomes (modified Rankin Score=0) despite no immunotherapy. These outcomes were superior to those of immunotherapy-treated patients with confirmed autoantibody-mediated encephalitis (p<0.05).
Conclusions: Seizure semiology, cognitive and mood phenotypes, alongside inflammatory investigation findings, aid the identification of surface autoantibodies among unselected people with new-onset focal epilepsy. The excellent immunotherapy-independent outcomes of autoantibody-positive patients without encephalitis suggests immunotherapy administration should be guided by clinical features of encephalitis, rather than autoantibody positivity. Our findings suggest that, in this cohort, immunotherapy-responsive seizure syndromes with autoantibodies largely fall under the umbrella of autoimmune encephalitis.
Keywords: autoimmune encephalitis; epilepsy; neuroimmunology.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: SRI and PW are coapplicants and receive royalties on patent application WO/210/046716 (UK patent no. PCT/GB2009/051441) entitled ‘Neurological Autoimmune Disorders’. The patent has been licensed for the development of assays for LGI1 and other VGKC-complex antibodies.
Figures
Comment in
-
Antineuronal antibodies and epilepsy: treat the patient, not the lab.J Neurol Neurosurg Psychiatry. 2021 Mar;92(3):230. doi: 10.1136/jnnp-2020-325350. Epub 2021 Jan 5. J Neurol Neurosurg Psychiatry. 2021. PMID: 33402418 Free PMC article. No abstract available.
-
The Search for Autoimmune-Associated Epilepsy Continues-Are We Getting Closer to Our Target?Epilepsy Curr. 2021 Apr 23;21(4):255-257. doi: 10.1177/15357597211010816. eCollection 2021 Jul-Aug. Epilepsy Curr. 2021. PMID: 34690560 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources