

An enhanced isothermal amplification assay for viral detection
- PMID: 33219228
- PMCID: PMC7679446
- DOI: 10.1038/s41467-020-19258-y
An enhanced isothermal amplification assay for viral detection
Abstract
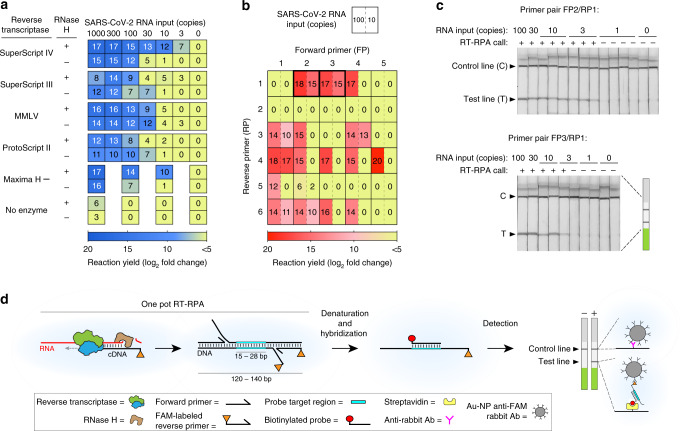
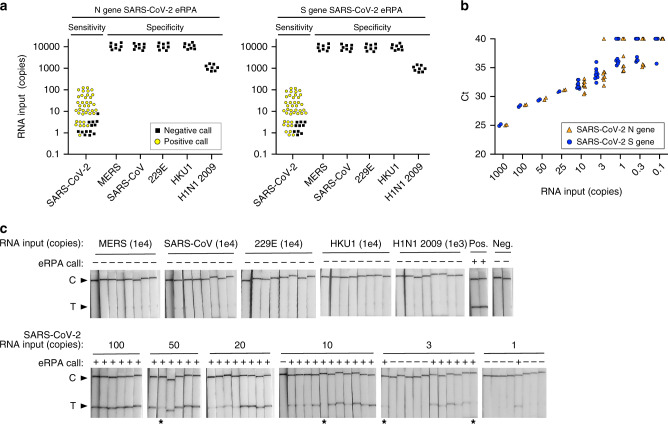
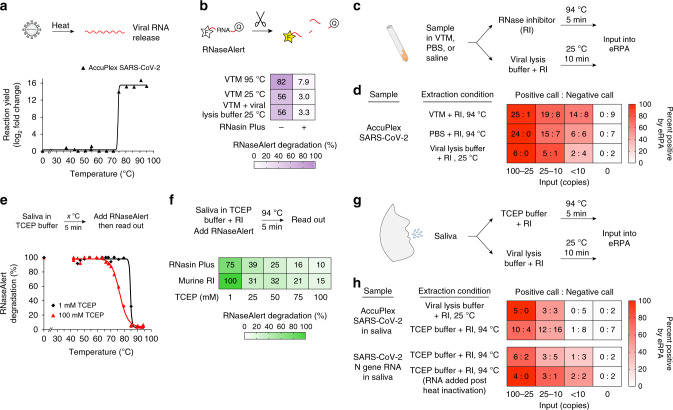
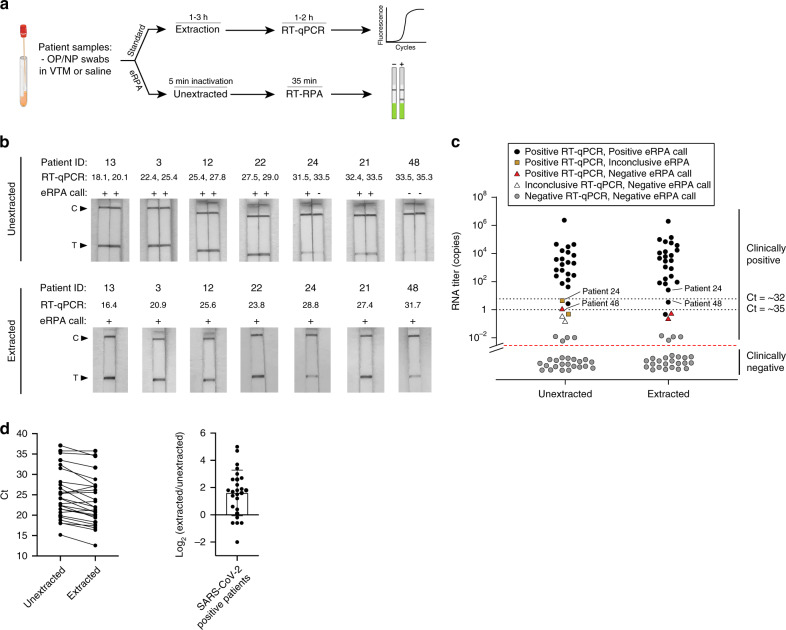
Rapid, inexpensive, robust diagnostics are essential to control the spread of infectious diseases. Current state of the art diagnostics are highly sensitive and specific, but slow, and require expensive equipment. Here we report the development of a molecular diagnostic test for SARS-CoV-2 based on an enhanced recombinase polymerase amplification (eRPA) reaction. eRPA has a detection limit on patient samples down to 5 viral copies, requires minimal instrumentation, and is highly scalable and inexpensive. eRPA does not cross-react with other common coronaviruses, does not require RNA purification, and takes ~45 min from sample collection to results. eRPA represents a first step toward at-home SARS-CoV-2 detection and can be adapted to future viruses within days of genomic sequence availability.
Conflict of interest statement
M.S. is inventor on U.S. Provisional Patent Application 63/993,521 and 63/031,120 (Harvard Case #8152). A company, Qtection LLC, has been launched to commercialize eRPA and provide effective testing options to the public. M.S. is a founder of the company. All other authors declare no competing interests.
Figures
Update of
-
An enhanced isothermal amplification assay for viral detection.bioRxiv [Preprint]. 2020 May 29:2020.05.28.118059. doi: 10.1101/2020.05.28.118059. bioRxiv. 2020. Update in: Nat Commun. 2020 Nov 20;11(1):5920. doi: 10.1038/s41467-020-19258-y. PMID: 32577657 Free PMC article. Updated. Preprint.
References
-
- Park, A. Dr. Anthony Fauci “not overly confident” with U.S. COVID-19 testing capabilities. time.comanthony-fauci-covid–testing-capabilities. Accessed 24 May 2020.
-
- Temple, J. Why contact tracing may be a mess in America. Accessed 24 May 2020.
-
- Srivatsan, S. et al. Preliminary support for a ‘dry swab, extraction free’ protocol for SARS-CoV-2 testing via RT-qPCR. bioRxiv10.1101/2020.04.22.056283 (2020).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
