

Clinical charts for surveillance of growth and body proportion development in achondroplasia and examples of their use
- PMID: 33220165
- PMCID: PMC7839678
- DOI: 10.1002/ajmg.a.61974
Clinical charts for surveillance of growth and body proportion development in achondroplasia and examples of their use
Abstract
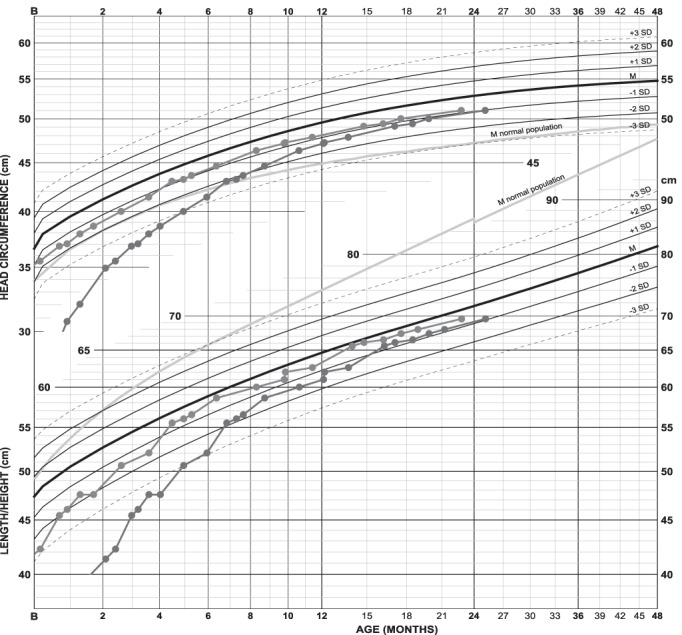
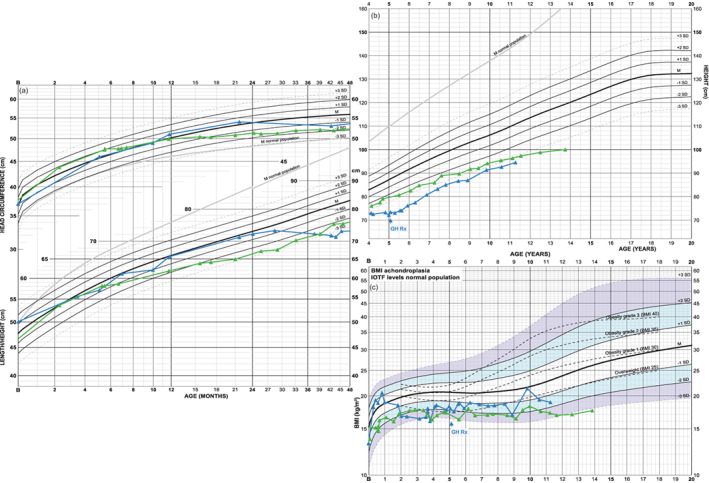
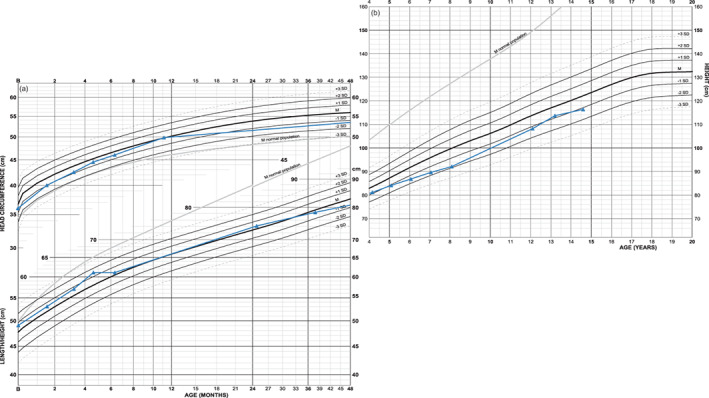
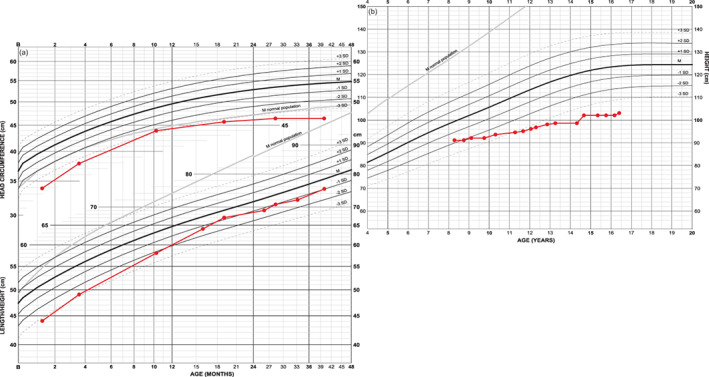
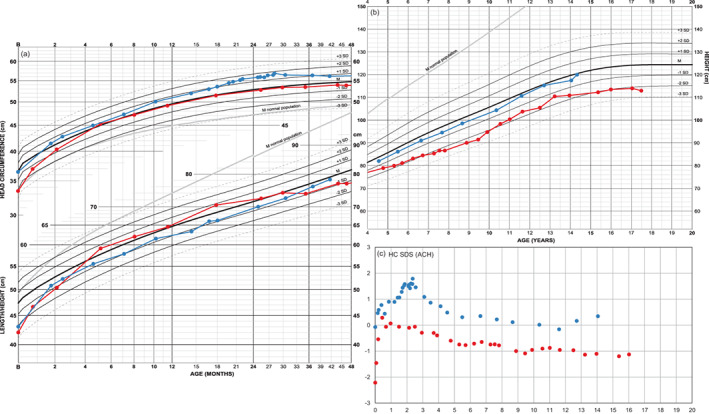
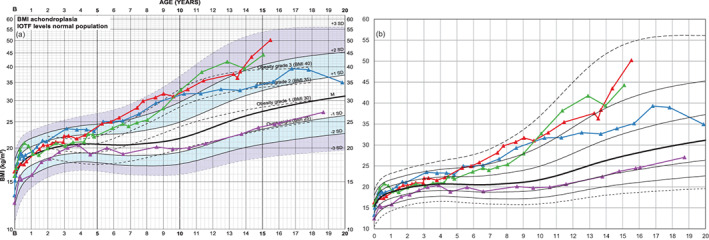
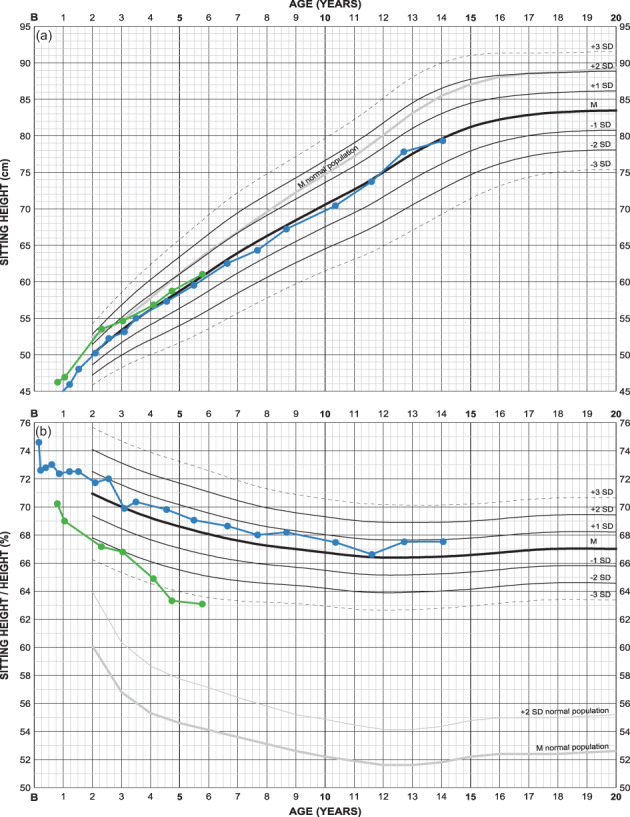
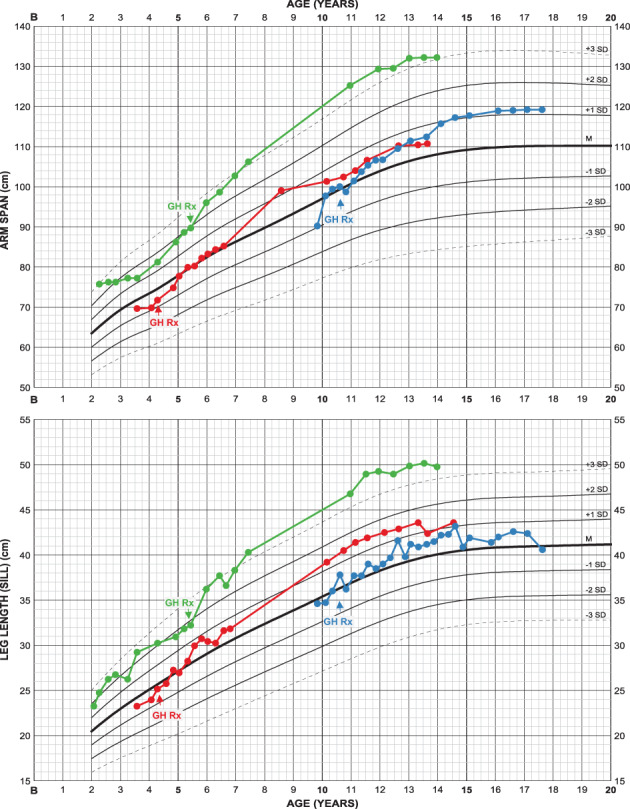
Clinical surveillance of infants and children with achondroplasia necessitates syndrome-specific charts due to extreme short stature with deviating body proportions. Height, arm span and leg length develop far below normal population ranges. We present growth and body proportion charts for ages 0-20 years, constructed from semi-longitudinal standardized measurements of about 450 children, along with some examples of achondroplasia typical and atypical growth pattern. We combine head circumference, height and weight for 0-4 years into one (infancy) page and height and weight for 4-20 years in another (childhood-adolescence) using nonlinear axes to account for the rapidly decreasing growth velocity. Similarly, weight and BMI are based on nonlinear axes to balance wide SD-channels at higher and narrow SD-channels at lower levels of weight/BMI. Charts for following sitting height, sitting height/height ratio, arm span, leg and foot length are also presented. Clinical examples illustrating the applicability of the charts include cases of extreme prematurity, extreme head circumference development before and after shunting, achondroplasia complicated by chromosomal or additional genetic abnormality and by growth hormone deficiency as well as of evaluating growth promoting therapy.
Keywords: achondroplasia; clinical surveillance; growth chart.
© 2020 The Authors. American Journal of Medical Genetics Part A published by Wiley Periodicals LLC.
Conflict of interest statement
Lars Hagenäs has received a research grant and consultant fee from BioMarin Europe Ltd. and has received consultant fee from Ascendis Inc.
Figures
References
-
- Arditi, J. D. , Thomaidis, L. , Frysira, H. , Doulgeraki, A. , Chrousos, G. P. , & Kanaka‐Gantenbein, C. (2017, July). Long‐term follow‐up of a child with Klinefelter syndrome and achondroplasia from infancy to 16 years. Journal of Pediatric Endocrinology & Metabolism: JPEM, 30, 797–803. 10.1515/jpem-2016-0362 - DOI - PubMed
-
- Cole, T. J. , Freeman, J. V. , & Preece, M. A. (1998). British 1990 growth reference centiles for weight, height, body mass index and head circumference fitted by maximum penalized likelihood. Statistics in Medicine, 17(4), 407–429. - PubMed
-
- Cole, T. J. , & Green, P. J. (1992). Smoothing reference centile curves: The LMS method and penalized likelihood. Statistics in Medicine, 11(10), 1305–1319. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
