

Nonalcoholic fatty liver disease (NAFLD) from pathogenesis to treatment concepts in humans
- PMID: 33220492
- PMCID: PMC8324683
- DOI: 10.1016/j.molmet.2020.101122
Nonalcoholic fatty liver disease (NAFLD) from pathogenesis to treatment concepts in humans
Abstract
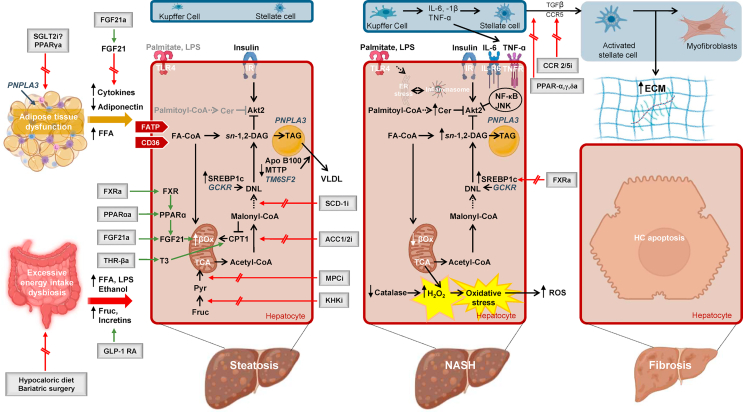
Background: Nonalcoholic fatty liver disease (NAFLD) comprises hepatic alterations with increased lipid accumulation (steatosis) without or with inflammation (nonalcoholic steatohepatitis, NASH) and/or fibrosis in the absence of other causes of liver disease. NAFLD is developing as a burgeoning health challenge, mainly due to the worldwide obesity and diabetes epidemics.
Scope of review: This review summarizes the knowledge on the pathogenesis underlying NAFLD by focusing on studies in humans and on hypercaloric nutrition, including effects of saturated fat and fructose, as well as adipose tissue dysfunction, leading to hepatic lipotoxicity, abnormal mitochondrial function, and oxidative stress, and highlights intestinal dysbiosis. These mechanisms are discussed in the context of current treatments targeting metabolic pathways and the results of related clinical trials.
Major conclusions: Recent studies have provided evidence that certain conditions, for example, the severe insulin-resistant diabetes (SIRD) subgroup (cluster) and the presence of an increasing number of gene variants, seem to predispose for excessive risk of NAFLD and its accelerated progression. Recent clinical trials have been frequently unsuccessful in halting or preventing NAFLD progression, perhaps partly due to including unselected cohorts in later stages of NAFLD. On the basis of this literature review, this study proposed screening in individuals with the highest genetic or acquired risk of disease progression, for example, the SIRD subgroup, and developing treatment concepts targeting the earliest pathophysiolgical alterations, namely, adipocyte dysfunction and insulin resistance.
Keywords: Clinical trials; Fatty liver; Fibrosis; Inflammation; Insulin resistance; Lipotoxicity.
Copyright © 2020 The Authors. Published by Elsevier GmbH.. All rights reserved.
Figures
References
-
- Cotter T.G., Rinella M. Nonalcoholic fatty liver disease 2020: the State of the disease. Gastroenterology. 2020;158:1851–1864. - PubMed
-
- Roden M. Mechanisms of disease: hepatic steatosis in type 2 diabetes-pathogenesis and clinical relevance. Nature Clinical Practice Endocrinology & Metabolism. 2006;2:335–348. - PubMed
-
- Pafili K., Maltezos E., Papanas N. Ipragliflozin and sodium glucose transporter 2 inhibitors to reduce liver fat: will the prize we sought be won? Expert Opinion on Pharmacotherapy. 2018;19:185–187. - PubMed
-
- Zaharia O.P., Strassburger K., Strom A., Bonhof G.J., Karusheva Y., Antoniou S. Risk of diabetes-associated diseases in subgroups of patients with recent-onset diabetes: a 5-year follow-up study. The Lancet Diabetes & Endocrinology. 2019;7:684–694. - PubMed
-
- Anstee Q.M., Targher G., Day C.P. Progression of NAFLD to diabetes mellitus, cardiovascular disease or cirrhosis. Nature Reviews Gastroenterology & Hepatology. 2013;10:330–344. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
