

Comparative Outcomes of Cap Assisted Endoscopic Resection and Endoscopic Submucosal Dissection in Dysplastic Barrett's Esophagus
- PMID: 33220523
- PMCID: PMC8128933
- DOI: 10.1016/j.cgh.2020.11.017
Comparative Outcomes of Cap Assisted Endoscopic Resection and Endoscopic Submucosal Dissection in Dysplastic Barrett's Esophagus
Abstract
Background & aims: Endoscopic resection is an important component of the endoscopic treatment of Barrett's esophagus (BE) with dysplasia and intramucosal adenocarcinoma. Endoscopic resection can be performed by cap-assisted endoscopic mucosal resection (cEMR) or endoscopic submucosal dissection (ESD). We compared the histologic outcomes of ESD vs cEMR, followed by ablation.
Methods: We queried a prospectively maintained database of all patients undergoing cEMR and ESD followed by ablation at our institution from January 2006 to March 2020 and abstracted relevant demographic and clinical data. Our primary outcomes included the rate of complete remission of dysplasia (CRD): absence of dysplasia on surveillance histology, and complete remission of intestinal metaplasia (CRIM): absence of intestinal metaplasia. Our secondary outcome included complication rates.
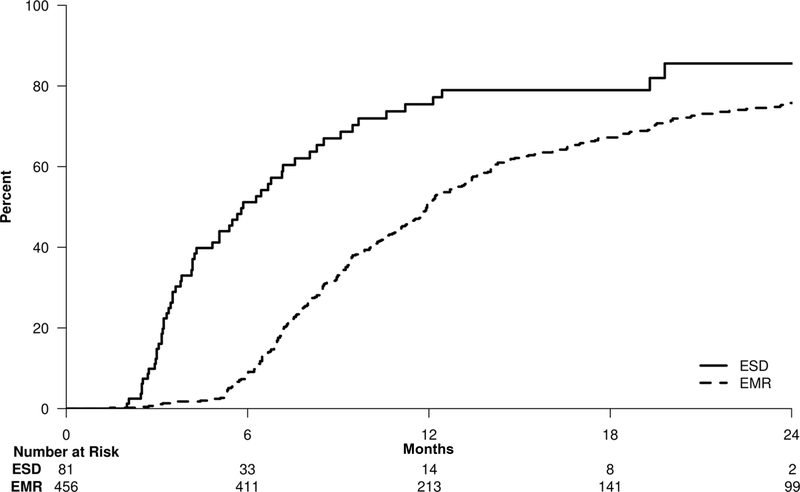
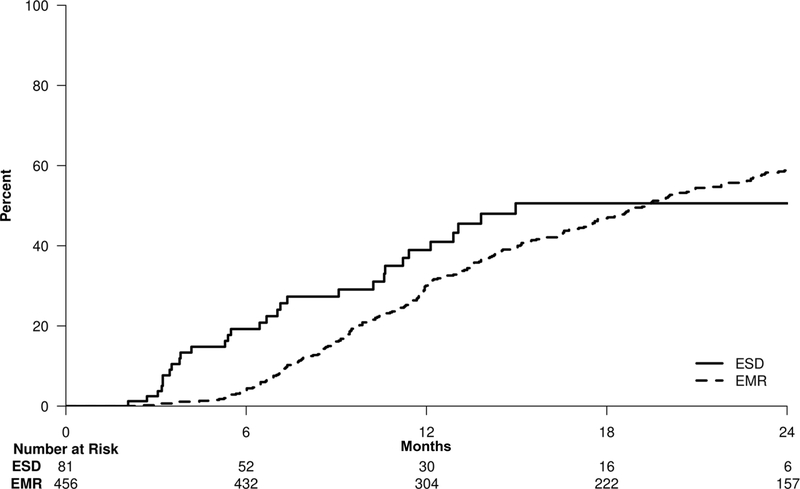
Results: We included 537 patients in the study: 456 underwent cEMR and 81 underwent ESD. The cumulative probabilities of CRD at 2 years were 75.8% and 85.6% in the cEMR and ESD groups, respectively (P < .01). Independent predictors of CRD were as follows: ESD (hazard ratio [HR], 2.38; P < .01) and shorter BE segment length (HR, 1.11; P < .01). The cumulative probabilities of CRIM at 2 years were 59.3% and 50.6% in the cEMR and ESD groups, respectively (P > .05). The only independent predictor of CRIM was a shorter BE segment (HR, 1.16; P < .01).
Conclusions: BE patients with dysplasia or intramucosal adenocarcinoma undergoing ESD reach CRD at higher rates than those treated with cEMR, although CRIM rates at 2 years and complication rates were similar between the 2 groups.
Keywords: Barrett’s Esophagus; Endoscopic Eradication Therapy; Endoscopic Mucosal Resection; Endoscopic Submucosal Dissection; Esophageal Adenocarcinoma.
Copyright © 2022 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Misuse of Cox Proportional Hazards Regression in Comparing ESD and EMR Outcomes: Hazard Rates Must Be Proportional.Clin Gastroenterol Hepatol. 2022 Dec;20(12):2928-2929. doi: 10.1016/j.cgh.2022.01.042. Epub 2022 Feb 2. Clin Gastroenterol Hepatol. 2022. PMID: 35121159 No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics,2019. CA Cancer J Clin 2019;69:7–34. - PubMed
-
- Wani S, Mathur SC, Curvers WL, et al. Greater Interobserver Agreement by Endoscopic Mucosal Resection Than Biopsy Samples in Barrett’s Dysplasia. Clinical Gastroenterology and Hepatology 2010;8:783–788.e2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
