

Bridging the age gap in breast cancer. Impacts of omission of breast cancer surgery in older women with oestrogen receptor positive early breast cancer. A risk stratified analysis of survival outcomes and quality of life
- PMID: 33220653
- PMCID: PMC7789991
- DOI: 10.1016/j.ejca.2020.10.015
Bridging the age gap in breast cancer. Impacts of omission of breast cancer surgery in older women with oestrogen receptor positive early breast cancer. A risk stratified analysis of survival outcomes and quality of life
Abstract
Background: Age-related breast cancer treatment variance is widespread with many older women having primary endocrine therapy (PET), which may contribute to inferior survival and local control. This propensity-matched study determined if a subgroup of older women may safely be offered PET.
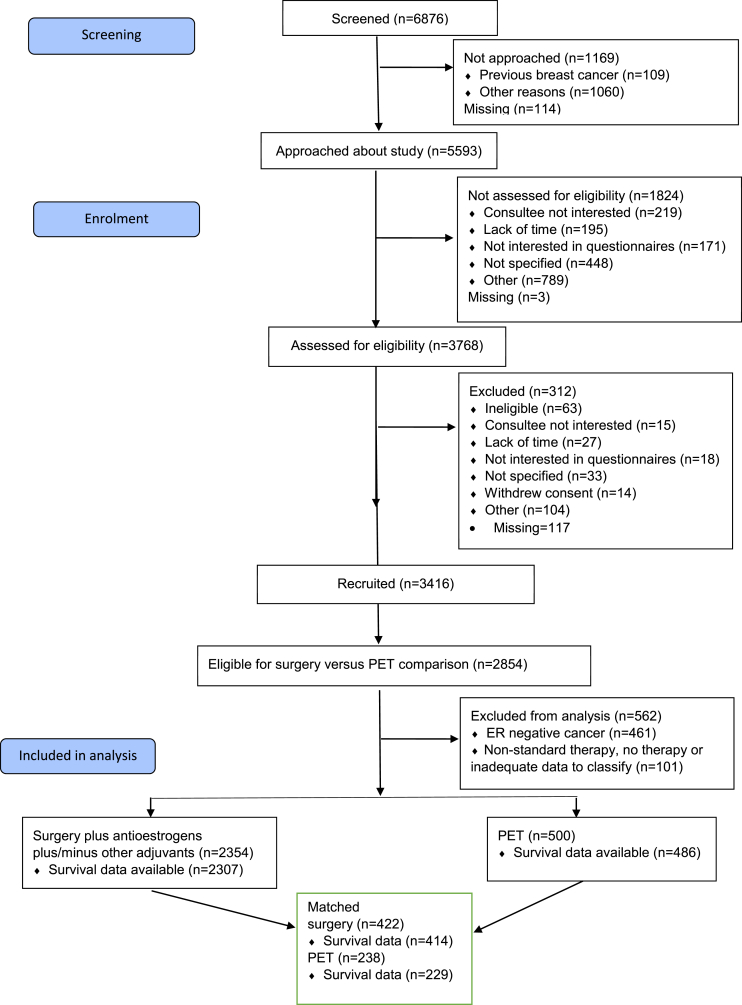
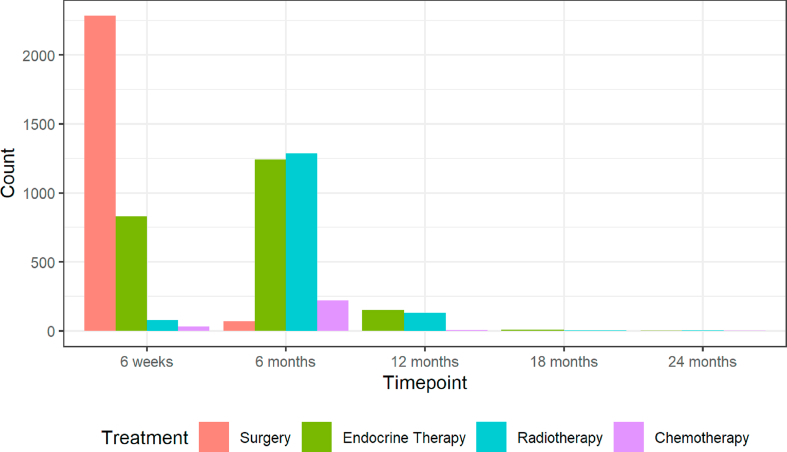
Methods: Multicentre, prospective, UK, observational cohort study with propensity-matched analysis to determine optimal allocation of surgery plus ET (S+ET) or PET in women aged ≥70 with breast cancer. Data on fitness, frailty, cancer stage, grade, biotype, treatment and quality of life were collected. Propensity-matching (based on age, health status and cancer stage) adjusted for allocation bias when comparing S+ET with PET.
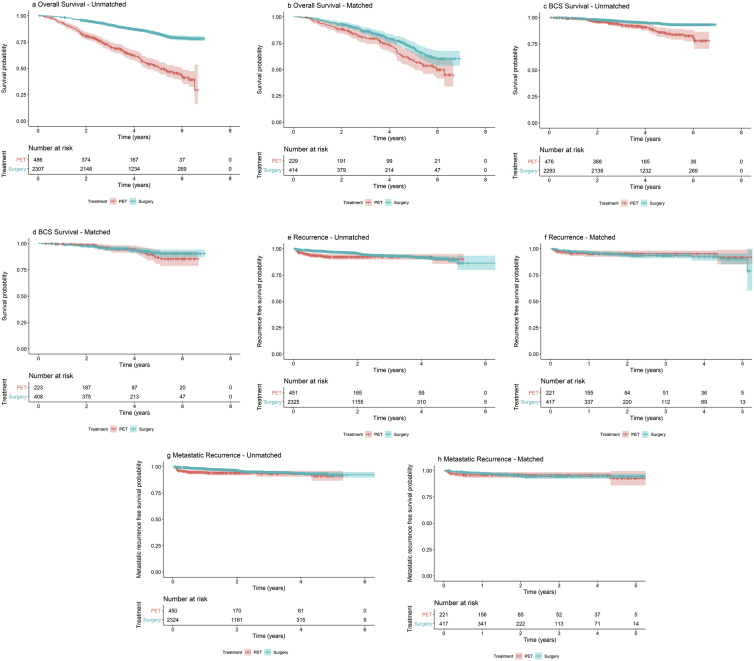
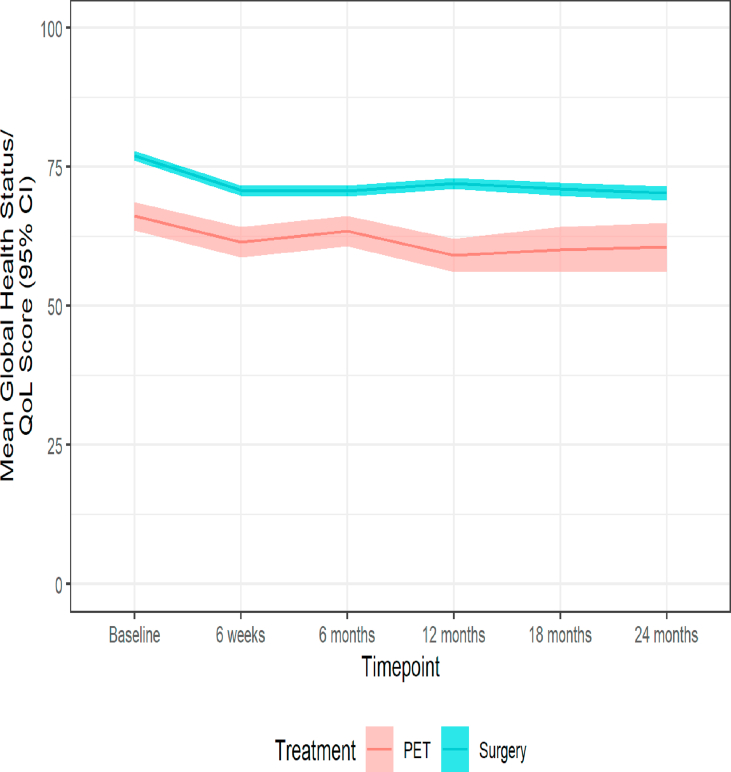
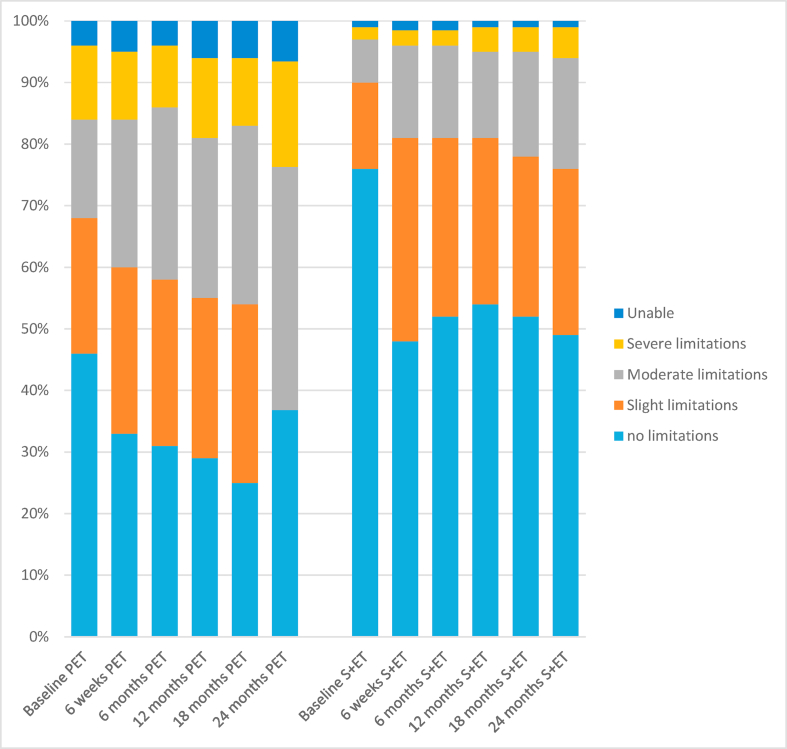
Findings: A total of 3416 women (median age 77, range 69-102) were recruited from 56 breast units-2854 (88%) had ER+ breast cancer: 2354 had S+ET and 500 PET. Median follow-up was 52 months. Patients treated with PET were older and frailer than patients treated with S+ET. Unmatched overall survival was inferior in the PET group (hazard ratio, (HR) 0.27, 95% confidence interval (CI) 0.23-0.33, P < 0.001). Unmatched breast cancer-specific survival (BCSS) was also inferior in patients treated with PET (HR: 0.41, CI: 0.29-0.58, P < 0.001 for BCSS). In the matched analysis, PET was still associated with an inferior overall survival (HR = 0.72, 95% CI: 0.53-0.98, P = 0.04) but not BCSS (HR = 0.74, 95% CI: 0.40-1.37, P = 0.34) although at 4-5 years subtle divergence of the curves commenced in favor of surgery. Global health status diverged at certain time points between groups but over 24 months was similar when adjusted for baseline variance.
Interpretation: For the majority of older women with early ER+ breast cancer, surgery is oncologically superior to PET. In less fit, older women, with characteristics similar to the matched cohort of this study (median age 81 with higher comorbidity and functional impairment burdens, the BCSS survival differential disappears at least out to 4-5 year follow-up, suggesting that for those with less than 5-year predicted life-expectancy (>90 years or >85 with comorbidities or frailty) individualised decision making regarding PET versus S+ET may be appropriate and safe to offer. The Age Gap online decision tool may support this decision-making process (https://agegap.shef.ac.uk/).
Trial registration number: ISRCTN: 46099296.
Keywords: Adjuvant endocrine therapy; Breast cancer; Older women; Patient-centred outcomes; Primary endocrine therapy; Propensity score matching; Quality of life; Surgery; Survival.
Copyright © 2020 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Conflict of interest statement None declared.
Figures
References
-
- Diab S.G., Elledge R.M., Clark G.M. Tumor characteristics and clinical outcome of elderly women with breast cancer. J Natl Cancer Inst. 2000;92(7):550–556. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
