

Prognosis after surgery for multiple endocrine neoplasia type 1-related pancreatic neuroendocrine tumors: Functionality matters
- PMID: 33220975
- PMCID: PMC9263962
- DOI: 10.1016/j.surg.2020.09.037
Prognosis after surgery for multiple endocrine neoplasia type 1-related pancreatic neuroendocrine tumors: Functionality matters
Abstract
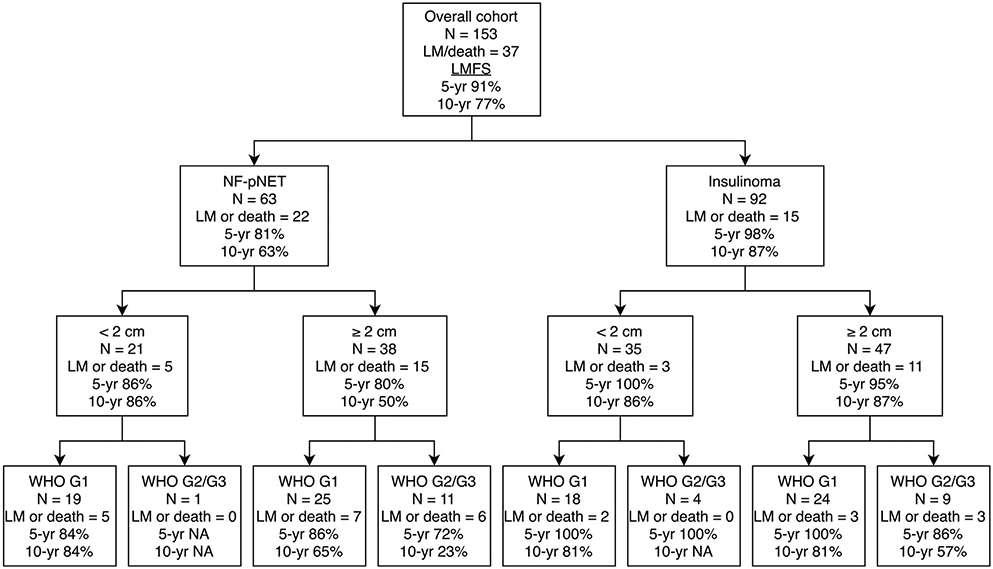
Background: Metastasized pancreatic neuroendocrine tumors are the leading cause of death in patients with multiple endocrine neoplasia type 1. Aside from tumor size, prognostic factors of pancreatic neuroendocrine tumors are largely unknown. The present study aimed to assess whether the prognosis of patients with resected multiple endocrine neoplasia type 1-related nonfunctioning pancreatic neuroendocrine tumors differs from those with resected multiple endocrine neoplasia type 1-related insulinomas and assessed factors associated with prognosis.
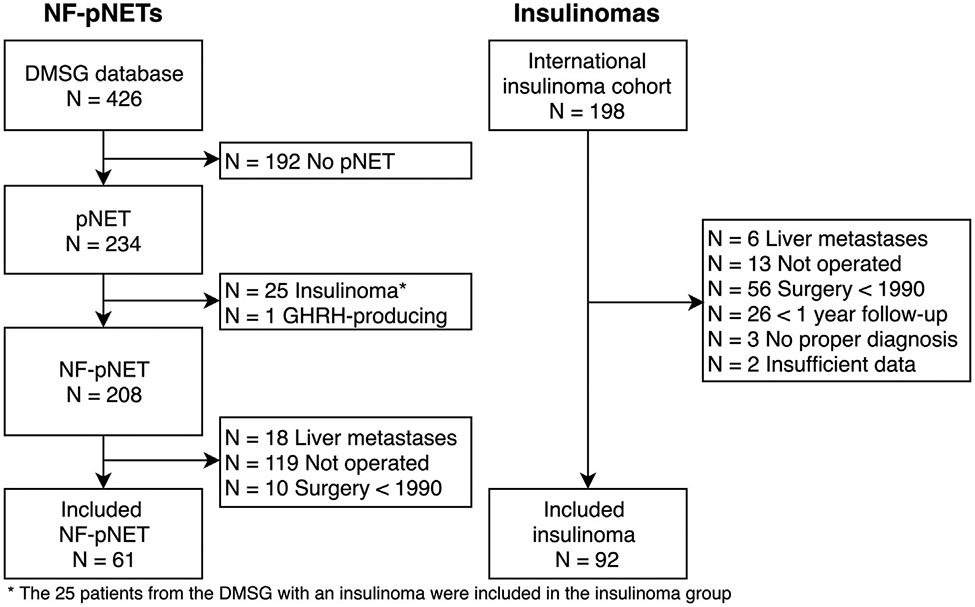
Methods: Patients who underwent resection of a multiple endocrine neoplasia type 1-related pancreatic neuroendocrine tumors between 1990 and 2016 were identified in 2 databases: the DutchMEN Study Group and the International MEN1 Insulinoma Study Group databases. Cox regression was performed to compare liver metastases-free survival of patients with a nonfunctioning pancreatic neuroendocrine tumors versus those with an insulinoma and to identify factors associated with liver metastases-free survival.
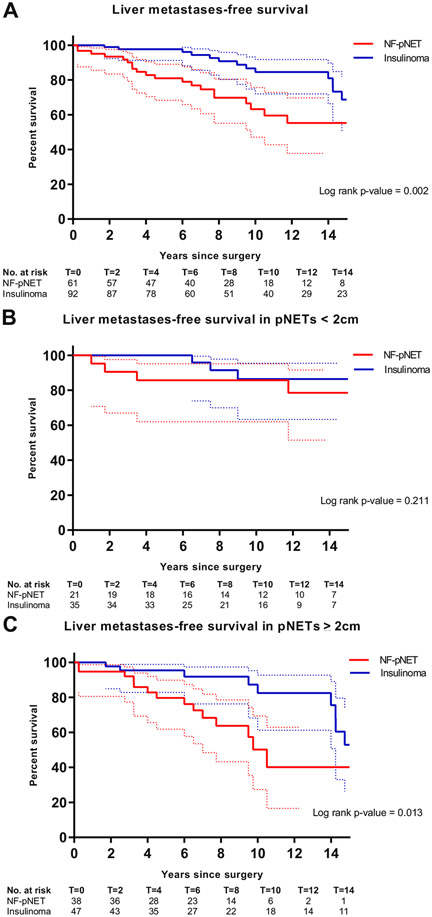
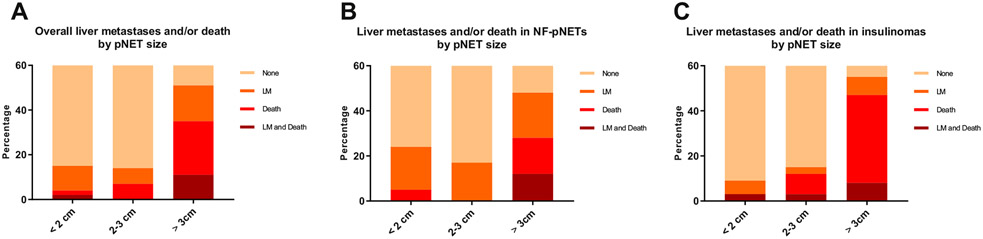
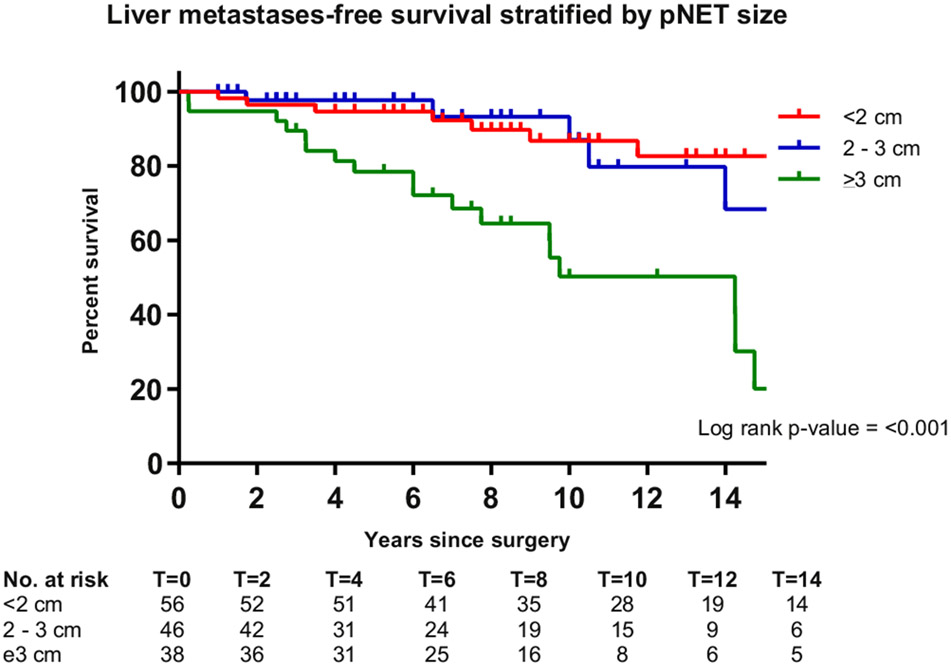
Results: Out of 153 patients with multiple endocrine neoplasia type 1, 61 underwent resection for a nonfunctioning pancreatic neuroendocrine tumor and 92 for an insulinoma. Of the patients with resected lymph nodes, 56% (18/32) of nonfunctioning pancreatic neuroendocrine tumors had lymph node metastases compared to 10% (4/41) of insulinomas (P = .001). Estimated 10-year liver metastases-free survival was 63% (95% confidence interval 42%-76%) for nonfunctioning pancreatic neuroendocrine tumors and 87% (72%-91%) for insulinomas. After adjustment for size, World Health Organization tumor grade, and age, nonfunctioning pancreatic neuroendocrine tumors had an increased risk for liver metastases or death (hazard ratio 3.04 [1.47-6.30]). In pancreatic neuroendocrine tumors ≥2 cm, nonfunctioning pancreatic neuroendocrine tumors (2.99 [1.22-7.33]) and World Health Organization grade 2 (2.95 [1.02-8.50]) were associated with liver metastases-free survival.
Conclusion: Patients with resected multiple endocrine neoplasia type 1-related nonfunctioning pancreatic neuroendocrine tumors had a significantly lower liver metastases-free survival than patients with insulinomas. Postoperative counseling and follow-up regimens should be tumor type specific and at least consider size and World Health Organization grade.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest/Disclosure
The authors have nothing to disclose.
Figures
Similar articles
-
Initiating Pancreatic Neuroendocrine Tumor (pNET) Screening in Young MEN1 Patients: Results From the DutchMEN Study Group.J Clin Endocrinol Metab. 2021 Nov 19;106(12):3515-3525. doi: 10.1210/clinem/dgab569. J Clin Endocrinol Metab. 2021. PMID: 34333645
-
What is the appropriate management of nonfunctioning pancreatic neuroendocrine tumours disclosed on screening in adult patients with multiple endocrine neoplasia type 1?Clin Endocrinol (Oxf). 2019 Dec;91(6):708-715. doi: 10.1111/cen.14094. Epub 2019 Oct 1. Clin Endocrinol (Oxf). 2019. PMID: 31505044 Review.
-
PROGNOSTIC FACTORS FOR SURVIVAL OF MEN1 PATIENTS WITH DUODENOPANCREATIC TUMORS METASTATIC TO THE LIVER: RESULTS FROM THE DMSG.Endocr Pract. 2017 Jun;23(6):641-648. doi: 10.4158/EP161639.OR. Epub 2017 Feb 22. Endocr Pract. 2017. PMID: 28225311
-
Penetrance of functioning and nonfunctioning pancreatic neuroendocrine tumors in multiple endocrine neoplasia type 1 in the second decade of life.J Clin Endocrinol Metab. 2014 Jan;99(1):E89-96. doi: 10.1210/jc.2013-1768. Epub 2013 Dec 20. J Clin Endocrinol Metab. 2014. PMID: 24178797
-
Surgery for gastrinoma and insulinoma in multiple endocrine neoplasia type 1.J Natl Compr Canc Netw. 2006 Feb;4(2):148-53. doi: 10.6004/jnccn.2006.0015. J Natl Compr Canc Netw. 2006. PMID: 16451771 Review.
Cited by
-
Blood-based Proteomic Signatures Associated With MEN1-related Duodenopancreatic Neuroendocrine Tumor Progression.J Clin Endocrinol Metab. 2023 Nov 17;108(12):3260-3271. doi: 10.1210/clinem/dgad315. J Clin Endocrinol Metab. 2023. PMID: 37307230 Free PMC article.
-
A Blood-based Polyamine Signature Associated With MEN1 Duodenopancreatic Neuroendocrine Tumor Progression.J Clin Endocrinol Metab. 2021 Nov 19;106(12):e4969-e4980. doi: 10.1210/clinem/dgab554. J Clin Endocrinol Metab. 2021. PMID: 34318891 Free PMC article.
-
Diagnosing pancreatic neuroendocrine tumors in patients with multiple endocrine neoplasia type 1 in daily practice.Front Endocrinol (Lausanne). 2022 Oct 7;13:926491. doi: 10.3389/fendo.2022.926491. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36277719 Free PMC article.
-
ASO Author Reflections: Severe Morbidity After Major Surgery in Patients with MEN1.Ann Surg Oncol. 2021 Aug;28(8):4400-4401. doi: 10.1245/s10434-020-09540-0. Epub 2021 Jan 27. Ann Surg Oncol. 2021. PMID: 33506308 Free PMC article. No abstract available.
-
Update on the clinical management of multiple endocrine neoplasia type 1.Clin Endocrinol (Oxf). 2022 Oct;97(4):409-423. doi: 10.1111/cen.14727. Epub 2022 Apr 1. Clin Endocrinol (Oxf). 2022. PMID: 35319130 Free PMC article. Review.
References
-
- Chandrasekharappa SC, Guru SC, Manickam P, et al. Positional cloning of the gene for multiple endocrine neoplasia-type 1. Science. 1997;276:404–407. - PubMed
-
- Lemmens I, Van de Ven WJ, Kas K, et al. Identification of the multiple endocrine neoplasia type 1 (MEN1) gene. The European Consortium on MEN1. Hum Mol Genet. 1997;6:1177–1183. - PubMed
-
- Goudet P, Murat A, Binquet C, et al. Risk factors and causes of death in MEN1 disease. A GTE (Groupe d’Etude des Tumeurs Endocrines) cohort study among 758 patients. World J Surg. 2010;34:249–255. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
