

Systemic and mucosal antibody responses specific to SARS-CoV-2 during mild versus severe COVID-19
- PMID: 33221383
- PMCID: PMC7677074
- DOI: 10.1016/j.jaci.2020.10.040
Systemic and mucosal antibody responses specific to SARS-CoV-2 during mild versus severe COVID-19
Abstract
Background: Whereas severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-specific antibody tests are increasingly being used to estimate the prevalence of SARS-CoV-2 infection, the determinants of these antibody responses remain unclear.
Objectives: Our aim was to evaluate systemic and mucosal antibody responses toward SARS-CoV-2 in mild versus severe coronavirus disease 2019 (COVID-19) cases.
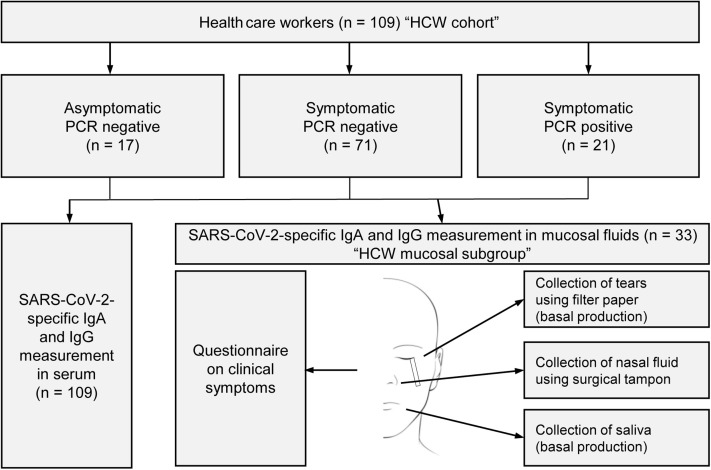
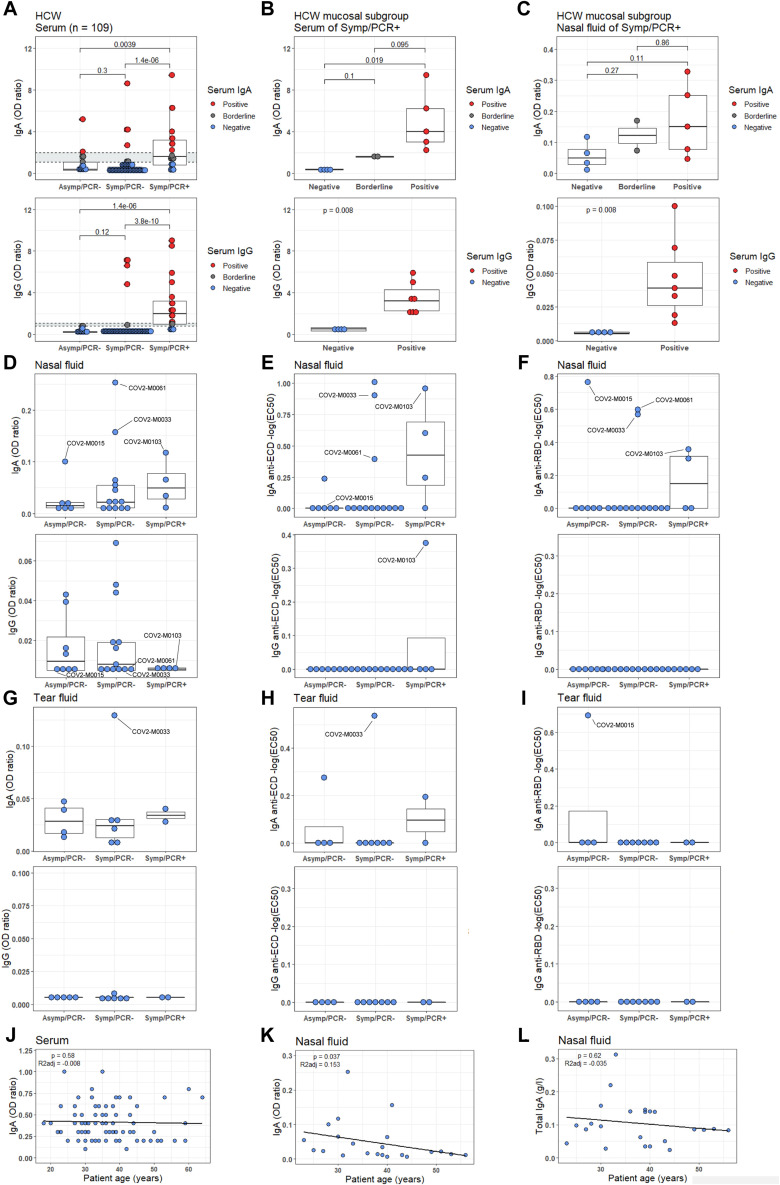
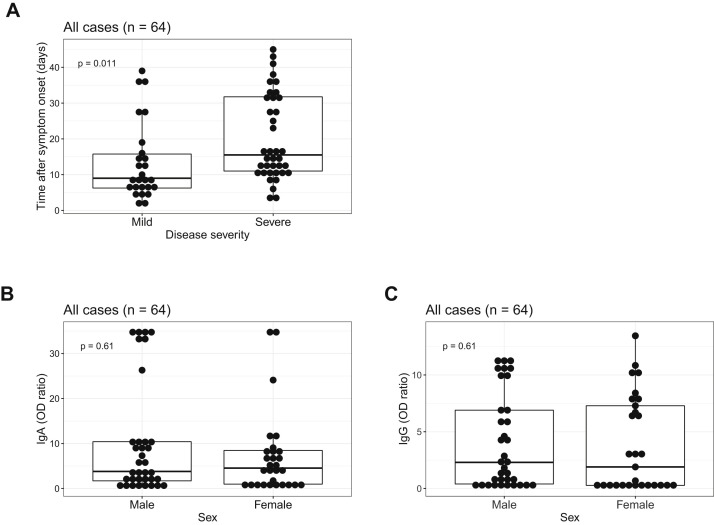
Methods: Using immunoassays specific for SARS-CoV-2 spike proteins, we determined SARS-CoV-2-specific IgA and IgG in sera and mucosal fluids of 2 cohorts, including SARS-CoV-2 PCR-positive patients (n = 64) and PCR-positive and PCR-negtive health care workers (n = 109).
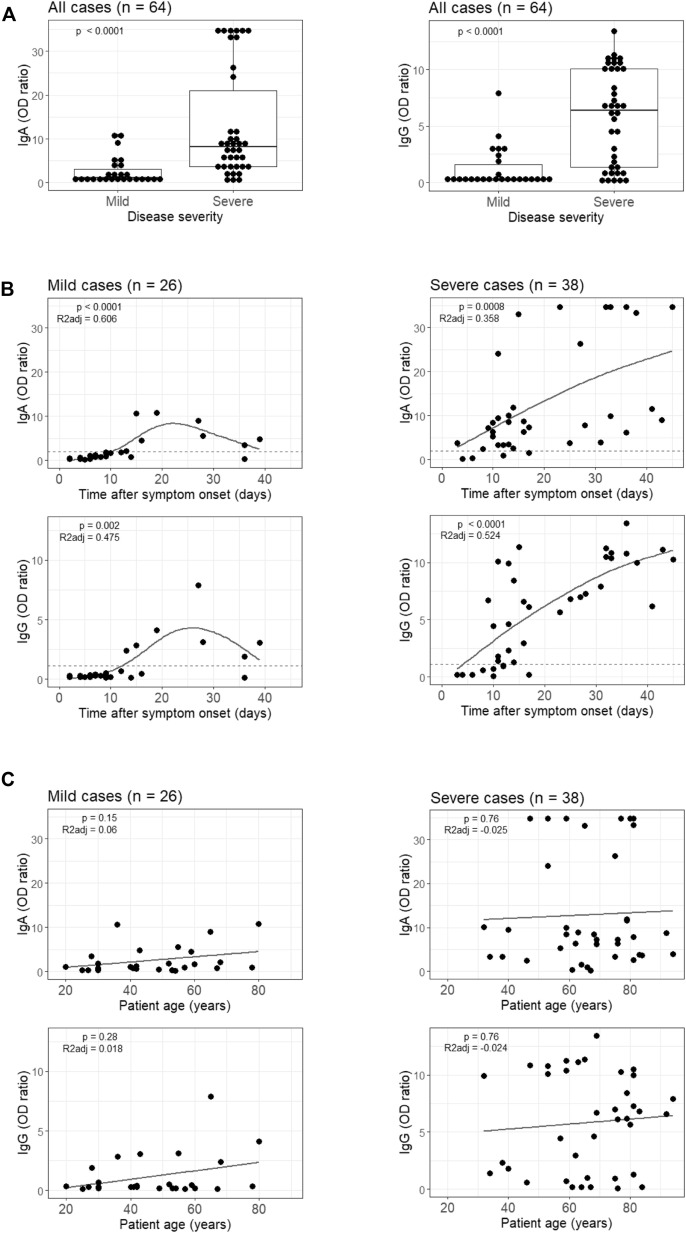
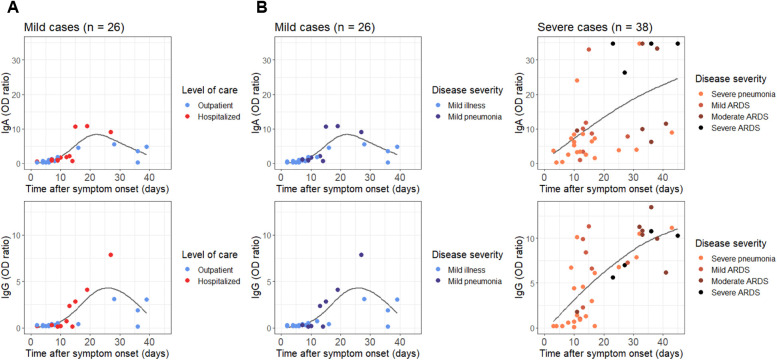
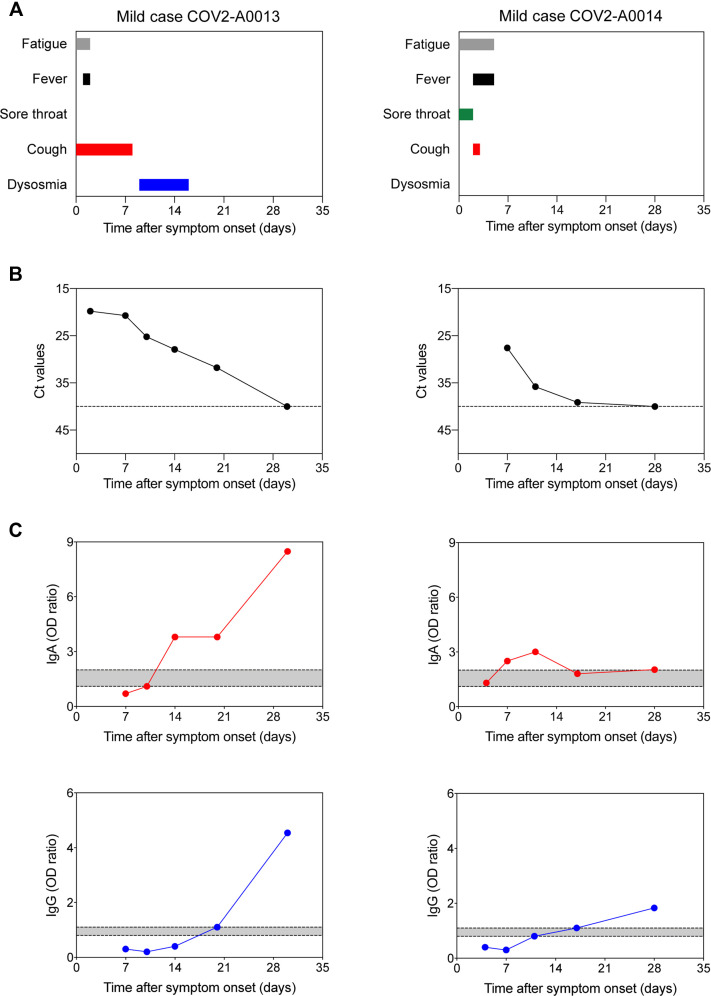
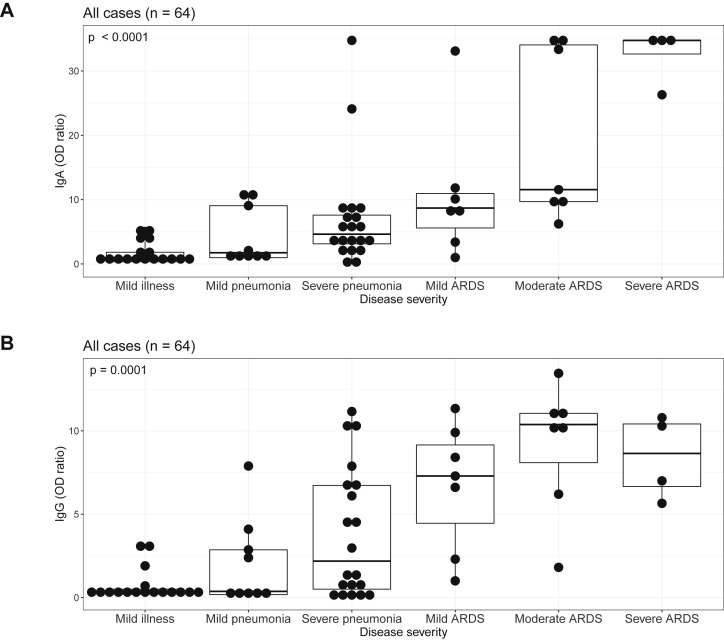
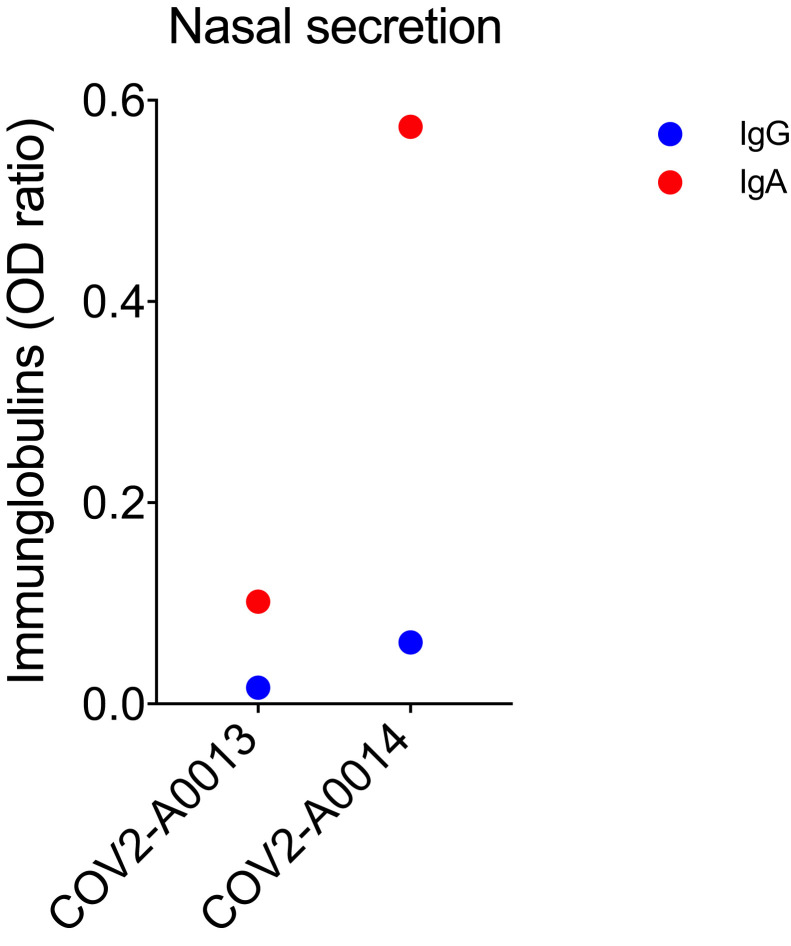
Results: SARS-CoV-2-specific serum IgA titers in patients with mild COVID-19 were often transiently positive, whereas serum IgG titers remained negative or became positive 12 to 14 days after symptom onset. Conversely, patients with severe COVID-19 showed a highly significant increase of SARS-CoV-2-specific serum IgA and IgG titers after symptom onset. Very high titers of SARS-CoV-2-specific serum IgA were correlated with severe acute respiratory distress syndrome. Interestingly, some health care workers with negative SARS-CoV-2-specific serum antibody titers showed SARS-CoV-2-specific IgA in mucosal fluids with virus-neutralizing capacity in some cases. SARS-CoV-2-specific IgA titers in nasal fluids were inversely correlated with age.
Conclusions: Systemic antibody production against SARS-CoV-2 develops mainly in patients with severe COVID-19, with very high IgA titers seen in patients with severe acute respiratory distress syndrome, whereas mild disease may be associated with transient production of SARS-CoV-2-specific antibodies but may stimulate mucosal SARS-CoV-2-specific IgA secretion.
Keywords: COVID-19; COVID-19 seroprevalence; COVID-19 severity; SARS-CoV-2; SARS-CoV-2–specific IgA; SARS-CoV-2–specific IgG; SARS-CoV-2–specific antibodies; humoral immune response; mucosal immune response.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures







References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
