

Benefits of robotically-assisted surgery for complex mitral valve repair
- PMID: 33221856
- PMCID: PMC8906674
- DOI: 10.1093/icvts/ivaa271
Benefits of robotically-assisted surgery for complex mitral valve repair
Abstract
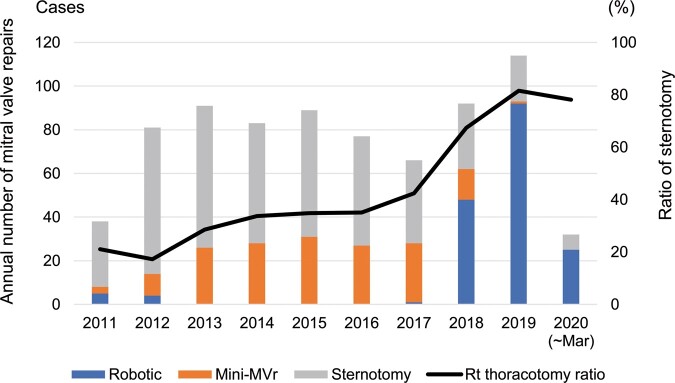
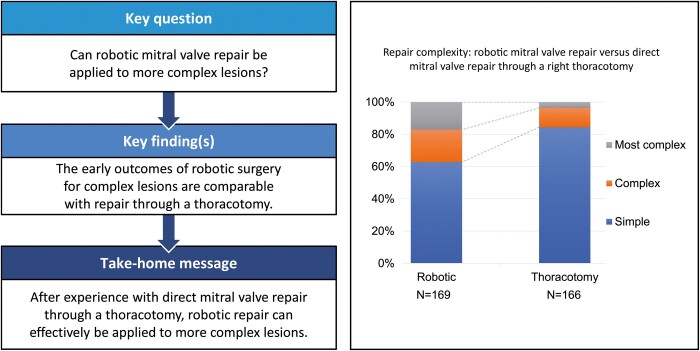
Objectives: To determine whether robotic mitral valve repair can be applied to more complex lesions compared with minimally invasive direct mitral valve repair through a right thoracotomy.
Methods: We enrolled 335 patients over a 9-year period; 95% of the robotic surgeries were performed after experience performing direct mitral valve repair.
Results: The mean age in the robotic versus thoracotomy repair groups was 61 ± 14 vs 55 ± 11 years, respectively (P < 0.001); 97% vs 100% of the patients, respectively, had degenerative aetiologies. Repair complexity was simple in 106 (63%) vs 140 (84%), complex in 34 (20%) vs 20 (12%) and most complex in 29 (17%) vs 6 (4%) patients undergoing robotic versus thoracotomy repair, respectively. The average complexity score with robotic repair was significantly higher versus thoracotomy repair (P < 0.001). The robotic group underwent more chordal replacement using polytetrafluoroethylene and less resections. All patients underwent ring annuloplasty. Cross-clamp time did not differ between the groups, and no strokes or deaths occurred. More patients undergoing robotic repair underwent concomitant procedures versus the thoracotomy group (30% vs 14%, respectively; P < 0.001). The overall repair rate was 100%, with no early mortality or strokes in either group. Postoperative mean residual mitral regurgitation was 0.3 in both groups, and the mean pressure gradient through the mitral valve was 2.4 vs 2.7 mmHg (robotic versus thoracotomy repair, respectively; P = 0.031).
Conclusions: Robotic surgery can be applied to repair more complex mitral lesions, with excellent early outcomes.
Keywords: Minimally invasive cardiac surgery; Mitral valve repair; Right thoracotomy; Robotic surgery.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures




References
-
- Nishi H, Miyata H, Motomura N, Toda K, Miyagawa S, Sawa Y. et al. Propensity-matched analysis of minimally invasive mitral valve repair using a nationwide surgical database. Surg Today 2015;45:1144–52. - PubMed
-
- Cosgrove DM, Sabik JF, Navia JL.. Minimally invasive valve operations. Ann Thorac Surg 1998;65:1535–9. - PubMed
-
- Lange R, Voss B, Kehl V, Mazzitelli D, Tassani-Prell P, Günther T.. Right minithoracotomy versus full sternotomy for mitral valve repair: propensity matched comparison. Ann Thorac Surg 2017;103:573–9. - PubMed
-
- Dogan S, Aybek T, Risteski PS, Detho F, Rapp A, Wimmer-Greinecker G. et al. Minimally invasive port access versus conventional mitral valve surgery: prospective randomized study. Ann Thorac Surg 2005;79:492–8. - PubMed
-
- Chitwood WR, Elbeery JR, Moran JF.. Minimally invasive mitral valve repair using transthoracic aortic occlusion. Ann Thorac Surg 1997;63:1477–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
