

Significance of Vertebral Body Sliding Osteotomy as a Surgical Strategy for the Treatment of Cervical Ossification of the Posterior Longitudinal Ligament
- PMID: 33222538
- PMCID: PMC9210231
- DOI: 10.1177/2192568220975387
Significance of Vertebral Body Sliding Osteotomy as a Surgical Strategy for the Treatment of Cervical Ossification of the Posterior Longitudinal Ligament
Abstract
Study design: Retrospective cohort study.
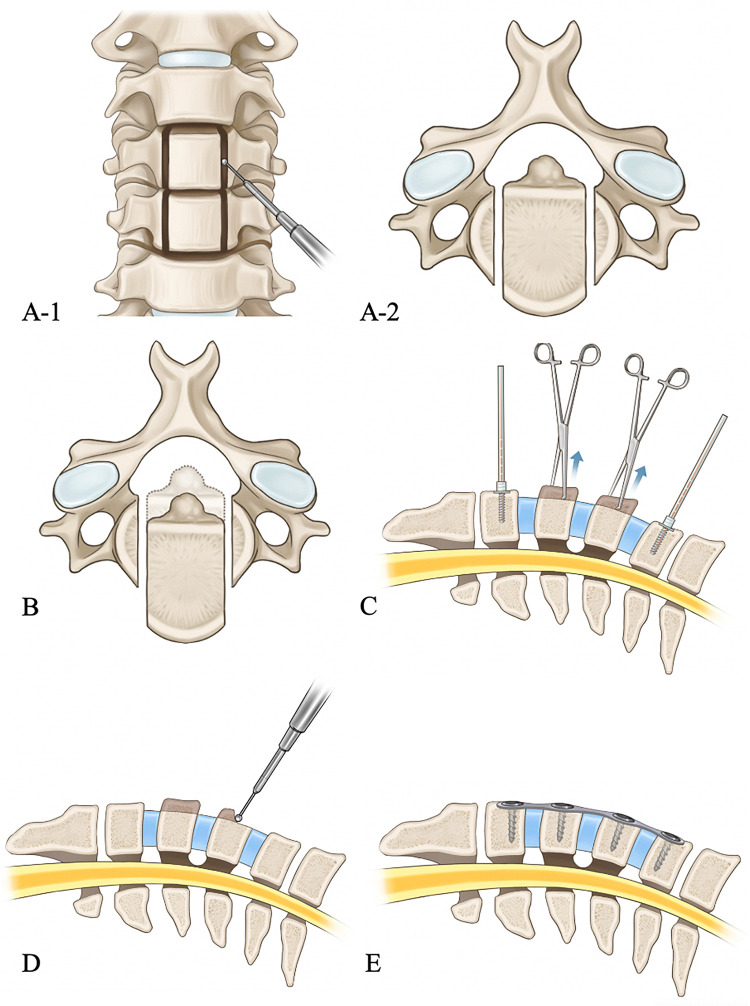
Objectives: Vertebral body sliding osteotomy (VBSO) has previously been reported as a technique to decompress ossification of the posterior longitudinal ligament (OPLL) by translating the vertebral body anteriorly. This study aimed to evaluate the radiological and clinical efficacies of VBSO and clarify the surgical indications of VBSO for treating myelopathy caused by OPLL.
Methods: Ninety-seven patients with symptomatic OPLL-induced cervical myelopathy treated with VBSO or laminoplasty who were followed up for more than 2 years were retrospectively reviewed. Cervical alignment, range of motion, fusion, modified K-line (mK-line) status, and minimum interval between ossified mass and mK-line (INT(min)), and the Japanese Orthopaedic Association (JOA) score were assessed. Patients in the VBSO group were compared with those who underwent laminoplasty.
Results: Cervical lordosis and INT(min) significantly increased in the VBSO group. All patients in the VBSO group assessed as mK-line (-) preoperatively were assessed as mK-line (+) postoperatively. However, in the LMP group, the mK-line status changed from (+) preoperatively to (-) postoperatively in 3 patients. Final JOA score (p = 0.02) and JOA score improvement (p = 0.01) were significantly higher in the VBSO group. JOA recovery ratio (p = 0.03) and proportion of patients with a recovery rate ≥50% were significantly higher in the VBSO group (p < 0.01).
Conclusions: VBSO is an effective surgical option for OPLL-induced myelopathy, demonstrating favorable neurological recovery and lordosis restoration with low complication rates. It is best indicated for kyphotic alignment, OPLL with a high space-occupying ratio, and OPLL involving ≤3 segments.
Keywords: K-line; anterior cervical corpectomy and fusion; cervical alignment; laminoplasty; ossification of posterior longitudinal ligament; vertebral body sliding osteotomy.
Conflict of interest statement
Figures




References
-
- Matsunaga S, Sakou T, Taketomi E, Komiya S. Clinical course of patients with ossification of the posterior longitudinal ligament: a minimum 10-year cohort study. J Neurosurg. 2004;100(3 Suppl Spine):245–248. - PubMed
-
- Matsumoto M, Chiba K, Toyama Y. Surgical treatment of ossification of the posterior longitudinal ligament and its outcomes: posterior surgery by laminoplasty. Spine (Phila Pa 1976). 2012;37(5):E303–E308. - PubMed
-
- Ogawa Y, Chiba K, Matsumoto M, et al. Long-term results after expansive open-door laminoplasty for the segmental-type of ossification of the posterior longitudinal ligament of the cervical spine: a comparison with nonsegmental-type lesions. J Neurosurg Spine. 2005;3(3):198–204. - PubMed
-
- Sodeyama T, Goto S, Mochizuki M, Takahashi J, Moriya H. Effect of decompression enlargement laminoplasty for posterior shifting of the spinal cord. Spine (Phila Pa 1976). 1999;24(15):1527–1531; discussion 1531-1522. - PubMed
-
- Koda M, Mochizuki M, Konishi H, et al. Comparison of clinical outcomes between laminoplasty, posterior decompression with instrumented fusion, and anterior decompression with fusion for K-line (-) cervical ossification of the posterior longitudinal ligament. Eur Spine J. 2016;25(7):2294–2301. - PubMed
LinkOut - more resources
Full Text Sources
