

High Prevalence of Pericardial Involvement in College Student Athletes Recovering From COVID-19
- PMID: 33223496
- PMCID: PMC7641597
- DOI: 10.1016/j.jcmg.2020.10.023
High Prevalence of Pericardial Involvement in College Student Athletes Recovering From COVID-19
Abstract
Objectives: This study sought to explore the spectrum of cardiac abnormalities in student athletes who returned to university campus in July 2020 with uncomplicated coronavirus disease 2019 (COVID-19).
Background: There is limited information on cardiovascular involvement in young individuals with mild or asymptomatic COVID-19.
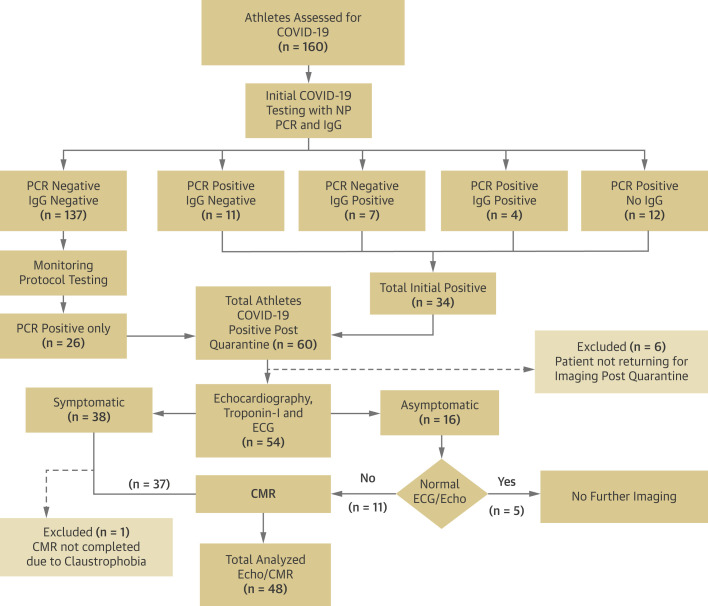
Methods: Screening echocardiograms were performed in 54 consecutive student athletes (mean age 19 years; 85% male) who had positive results of reverse transcription polymerase chain reaction nasal swab testing of the upper respiratory tract or immunoglobulin G antibodies against severe acute respiratory syndrome coronavirus type 2. Sequential cardiac magnetic resonance imaging was performed in 48 (89%) subjects.
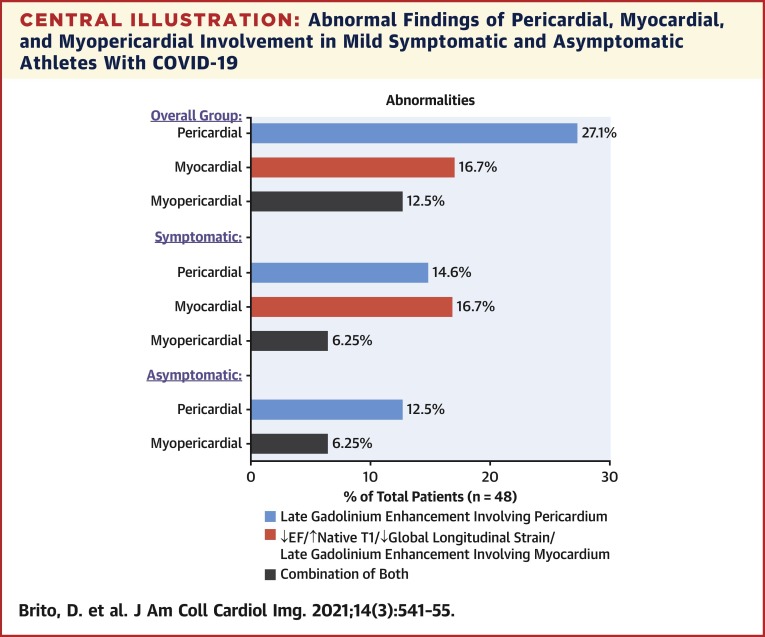
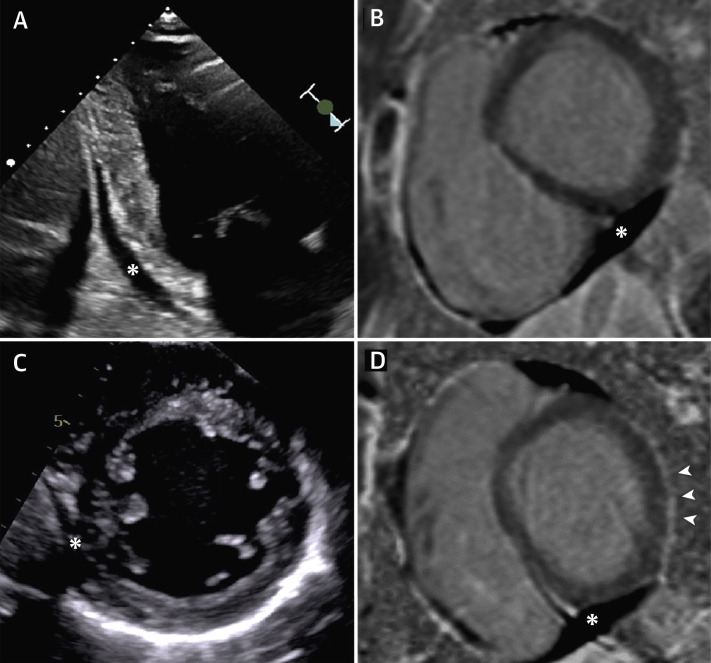
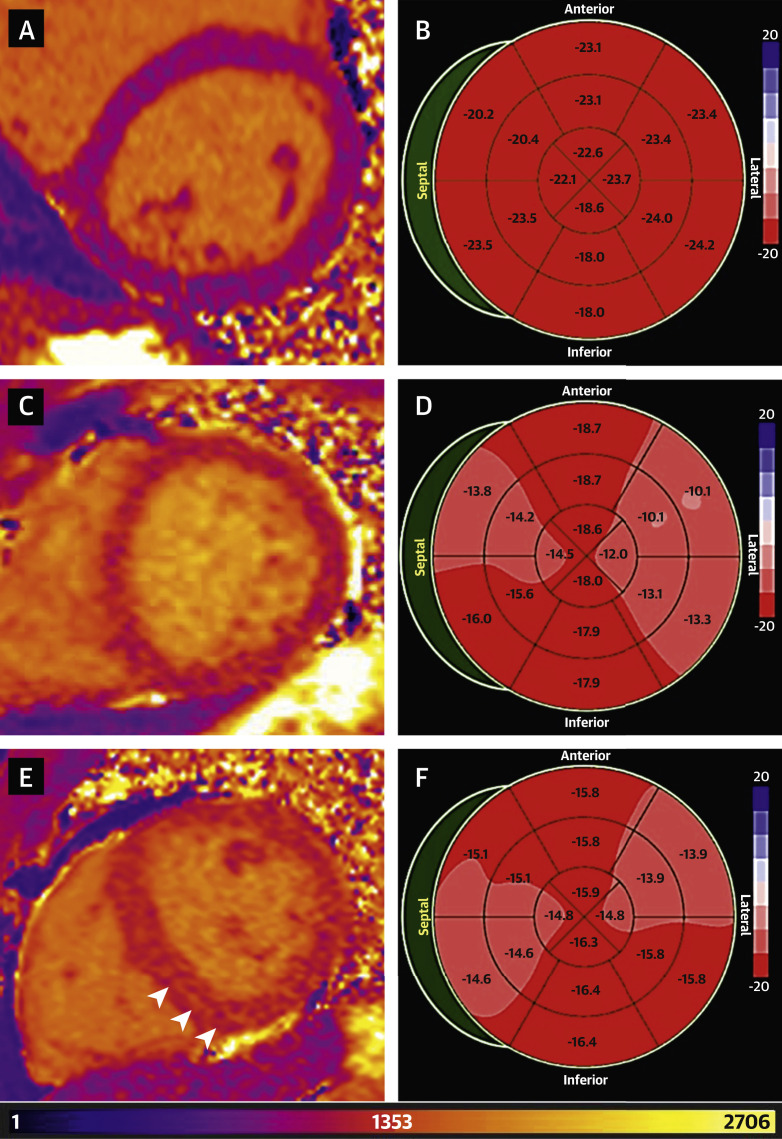
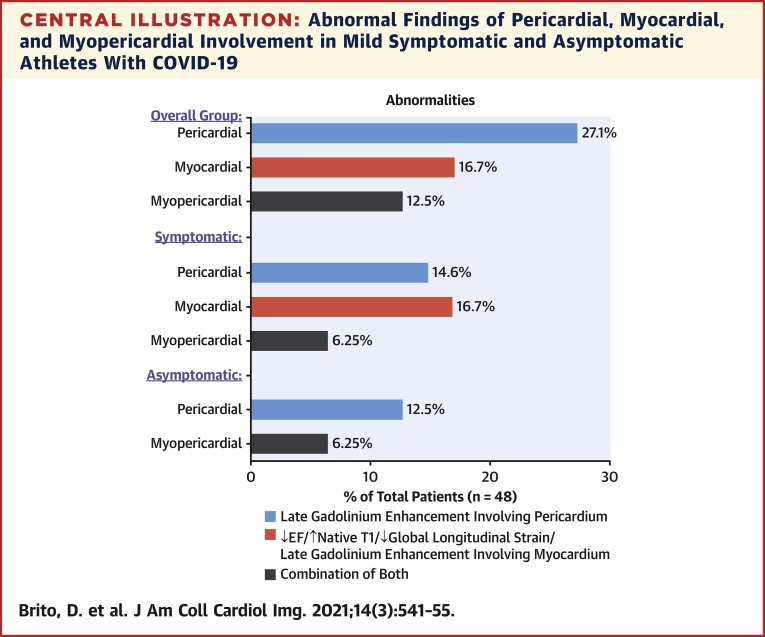
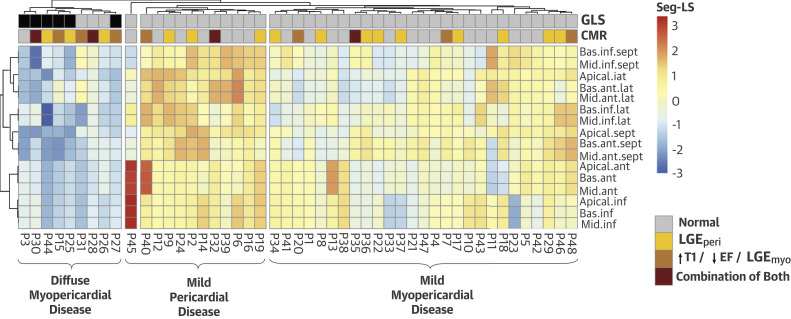
Results: A total of 16 (30%) athletes were asymptomatic, whereas 36 (66%) and 2 (4%) athletes reported mild and moderate COVID-19 related symptoms, respectively. For the 48 athletes completing both imaging studies, abnormal findings were identified in 27 (56.3%) individuals. This included 19 (39.5%) athletes with pericardial late enhancements with associated pericardial effusion. Of the individuals with pericardial enhancements, 6 (12.5%) had reduced global longitudinal strain and/or an increased native T1. One patient showed myocardial enhancement, and reduced left ventricular ejection fraction or reduced global longitudinal strain with or without increased native T1 values was also identified in an additional 7 (14.6%) individuals. Native T2 findings were normal in all subjects, and no specific imaging features of myocardial inflammation were identified. Hierarchical clustering of left ventricular regional strain identified 3 unique myopericardial phenotypes that showed significant association with the cardiac magnetic resonance findings (p = 0.03).
Conclusions: More than 1 in 3 previously healthy college athletes recovering from COVID-19 infection showed imaging features of a resolving pericardial inflammation. Although subtle changes in myocardial structure and function were identified, no athlete showed specific imaging features to suggest an ongoing myocarditis. Further studies are needed to understand the clinical implications and long-term evolution of these abnormalities in uncomplicated COVID-19.
Keywords: CMR; COVID-19; athletes; echocardiography; strain.
Copyright © 2021. Published by Elsevier Inc.
Conflict of interest statement
Funding Support and Author Disclosures This work is supported in part by funds from the National Science Foundation (NSF: # 1920920) National Institute of General Medical Sciences of the National Institutes of Health (NIH: #5U54GM104942-04). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the National Science Foundation. Dr. Sengupta has received consulting for HeartSciences, Kencor Health, and Ultromics. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Subclinical COVID-19 Cardiac Imaging Findings: Resurgence of the Athletic "Grey-Zone".JACC Cardiovasc Imaging. 2021 Mar;14(3):556-558. doi: 10.1016/j.jcmg.2020.12.005. Epub 2021 Jan 13. JACC Cardiovasc Imaging. 2021. PMID: 33454267 Free PMC article.
-
New Insights on COVID-19 and the Heart.JACC Cardiovasc Imaging. 2021 Mar;14(3):706-708. doi: 10.1016/j.jcmg.2021.01.010. JACC Cardiovasc Imaging. 2021. PMID: 33663773 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
