

Development and Validation of a Disease-Specific Oromandibular Dystonia Rating Scale (OMDRS)
- PMID: 33224096
- PMCID: PMC7669987
- DOI: 10.3389/fneur.2020.583177
Development and Validation of a Disease-Specific Oromandibular Dystonia Rating Scale (OMDRS)
Abstract
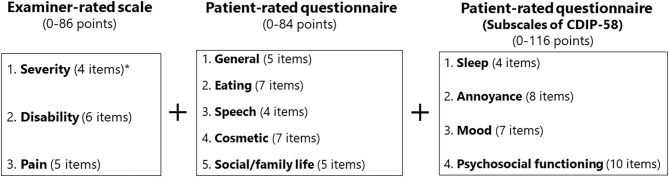
Background: Oromandibular dystonia manifests with sustained or task-specific contractions of the masticatory, tongue, and/or other muscles in the stomatognathic system. Since its symptoms can vary, it has been difficult to objectively measure disease severity and post-treatment changes. Objective: To develop and validate a comprehensive measurement tool for oromandibular dystonia. Methods: An examiner-rated scale included three subscales for severity, disability, and pain, modified specifically for oromandibular dystonia from the Toronto Western Spasmodic Torticollis Rating Scale-2. To evaluate the severity of each subtype of oromandibular dystonia, four of the six items were selected according to the subtype (jaw closing dystonia, tongue dystonia, jaw opening dystonia, jaw deviation [protrusion] dystonia, and lip dystonia). A patient-administered questionnaire based on clinical features and other relevant aspects associated with oromandibular dystonia was developed, which included five subscales: general, eating, speech, cosmetic, and social/family life. The questionnaire, examiner-rated scale, and four subscales (sleep, annoyance, mood, and psychosocial functioning) of the Cervical Dystonia Impact Profile-58 were combined to construct the oromandibular dystonia rating scale (OMDRS). The reliability and validity of the scale were assessed using clinimetric testing. Results: Six hundred and eighteen patients with oromandibular dystonia (394 women and 224 men; mean age, 51.7 years) were evaluated by the OMDRS. The overall OMDRS showed high-level internal consistency measured by Cronbach's alpha (0.95) with a logical factor structure. Cronbach's alpha for the subscales was satisfactory to excellent, ranging from 0.72 to 0.94. All items revealed acceptable inter-rater reliability (kappa > 0.4, interclass correlation coefficient > 0.6). Repeated ratings of videotapes revealed acceptable intra-rater reliability for all items (kappa > 0.76, interclass correlation coefficient > 0.86). Test-retest reliability showed a significant (p < 0.001) correlation efficiency. The OMDRS showed significant (p < 0.001) convergent and discriminant validity and significant (p < 0.001) sensitivity to changes after botulinum toxin therapy. Conclusion: The OMDRS can be useful for the comprehensive evaluation of disease severity, disability, psychosocial functioning, and impact on the quality of life as well as therapeutic changes in patients with oromandibular dystonia.
Keywords: Cervical Dystonia Impact Profile-58; Toronto Western Spasmodic Torticollis Rating Scale-2; disease severity; oromandibular dystonia; quality of life; rating scale; reliability; validity.
Copyright © 2020 Yoshida.
Figures

References
LinkOut - more resources
Full Text Sources