

Large Uterine Fibroids in Pregnancy with Successful Caesarean Myomectomy
- PMID: 33224543
- PMCID: PMC7671803
- DOI: 10.1155/2020/8880296
Large Uterine Fibroids in Pregnancy with Successful Caesarean Myomectomy
Abstract
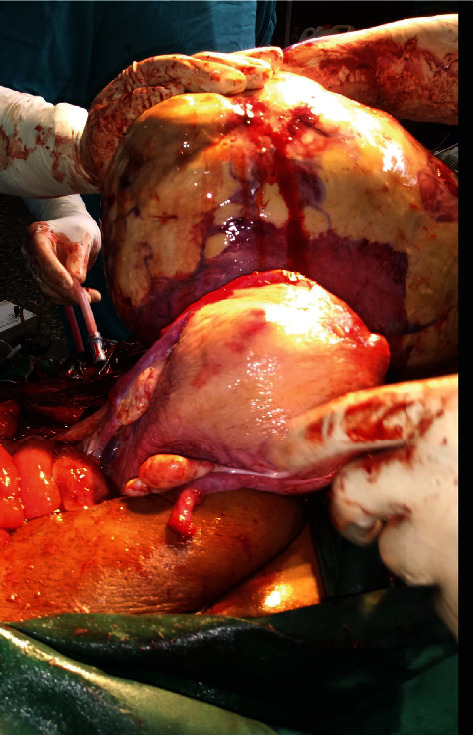
Uterine fibroid is the commonest benign tumour of the female reproductive tract. It occurs in 20-40% of women, whereas the estimated incidence in pregnancy is 0.1-3.9%. Uterine fibroid in pregnancy is usually asymptomatic with complications occurring in 10-30% of cases. The first line of management is conservative with counselling for myomectomy after delivery. However, in the presence of intractable symptoms, both antepartum myomectomy and caesarean myomectomy have been reported to be successfully performed in carefully selected cases. We report a case of large subserous uterine fibroid in pregnancy that was referred to our centre at 14 weeks of gestation. She developed generalized body weakness, backache, and breathlessness at 27 weeks gestation. Thus, she was admitted and managed conservatively for eight weeks with significant relief of symptoms. She eventually had a caesarean myomectomy at 35 weeks of gestation; the outcome was a live female baby with a birth weight of 2.3 kg and a large subserous fibroid weighing 9.5 kg. We can therefore say that caesarean myomectomy can be safely performed in carefully selected cases.
Copyright © 2020 Edu Eyong and Okon A. Okon.
Conflict of interest statement
The authors declare that there is no conflict of interests regarding the publication of this paper.
Figures


Similar articles
-
Innovative Management of a Giant Fibroid in Pregnancy: A Case Report.Cureus. 2024 Oct 5;16(10):e70894. doi: 10.7759/cureus.70894. eCollection 2024 Oct. Cureus. 2024. PMID: 39497893 Free PMC article.
-
Spontaneous complete regression of large uterine fibroid after the second vaginal delivery: Case report.Medicine (Baltimore). 2018 Nov;97(45):e13092. doi: 10.1097/MD.0000000000013092. Medicine (Baltimore). 2018. PMID: 30407315 Free PMC article.
-
Successful myomectomy during pregnancy: a case report.Reprod Health. 2005 Aug 16;2:6. doi: 10.1186/1742-4755-2-6. Reprod Health. 2005. PMID: 16105174 Free PMC article.
-
Conservative management of uterine artery pseudoaneurysm after laparoscopic-assisted myomectomy and subsequent pregnancy outcome: case series and review of the literature.Eur J Obstet Gynecol Reprod Biol. 2014 Nov;182:146-53. doi: 10.1016/j.ejogrb.2014.09.020. Epub 2014 Sep 19. Eur J Obstet Gynecol Reprod Biol. 2014. PMID: 25277771 Review.
-
Myoma and myomectomy: Poor evidence concern in pregnancy.J Obstet Gynaecol Res. 2017 Dec;43(12):1789-1804. doi: 10.1111/jog.13437. Epub 2017 Sep 11. J Obstet Gynaecol Res. 2017. PMID: 28892210 Review.
Cited by
-
Innovative Management of a Giant Fibroid in Pregnancy: A Case Report.Cureus. 2024 Oct 5;16(10):e70894. doi: 10.7759/cureus.70894. eCollection 2024 Oct. Cureus. 2024. PMID: 39497893 Free PMC article.
-
Huge Fibroid in Pregnancy: A Case Presentation.Cureus. 2024 May 3;16(5):e59566. doi: 10.7759/cureus.59566. eCollection 2024 May. Cureus. 2024. PMID: 38707757 Free PMC article.
References
-
- Panchal D. W., Doshi H. U., Singh P., Rohit P. Co-existing large fibroid in pregnancy: a case report. Gujarat Medical Journal. 2012;67(2):110–112.
Publication types
LinkOut - more resources
Full Text Sources
