

Cardiovascular risk and complications associated with COVID-19
- PMID: 33224599
- PMCID: PMC7675166
Cardiovascular risk and complications associated with COVID-19
Abstract
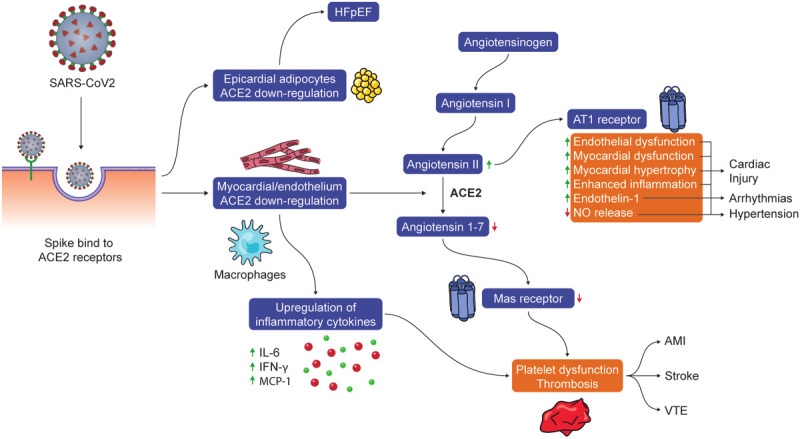
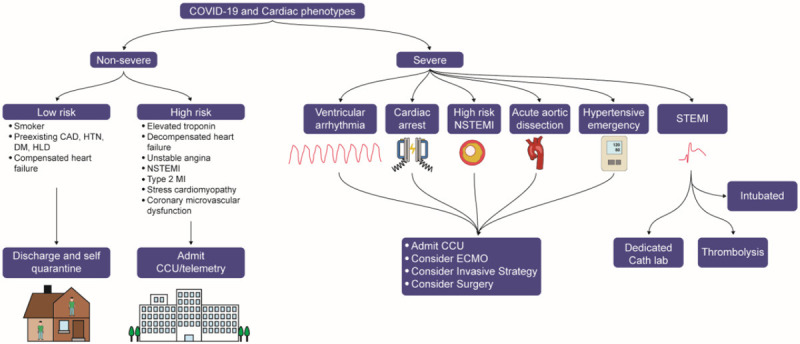
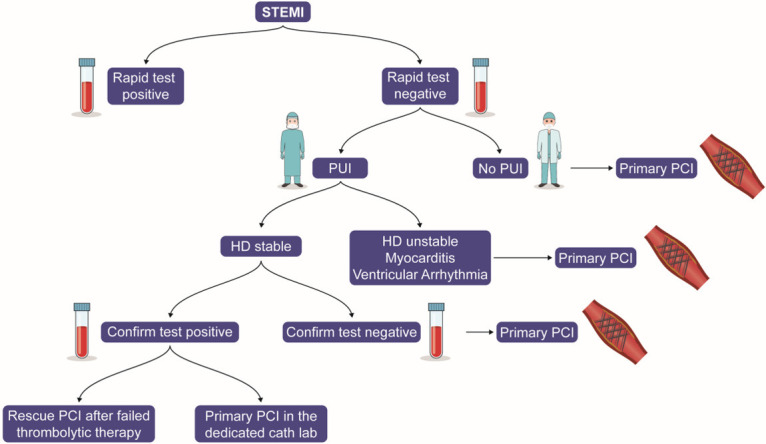
In December 2019, an unprecedented outbreak of pneumonia cases associated with acute respiratory distress syndrome (ARDS) first occurred in Wuhan, Hubei Province, China. The disease, later named Coronavirus disease 2019 (COVID-19) by the World Health Organization (WHO), was caused by the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2), and on January 30, 2020, the WHO declared the outbreak of COVID-19 to be a public health emergency. COVID-19 is now a global pandemic impacting more than 43,438,043 patients with 1,158,596 deaths globally as of August 26th, 2020. COVID-19 is highly contagious and has caused more deaths than SARS in 2002-2003 or the Middle East Respiratory Syndrome (MERS) in 2012-2013 combined and represents an unprecedented human affliction not seen since the influenza pandemic of 1918. COVID-19 has been associated with several cardiac complications, including hypercoagulability, acute myocardial injury and myocarditis, arrhythmias, and acute coronary syndromes. Patients with pre-existing cardiovascular disease (CVD) are at the highest risk for myocardial injury and mortality among infected patients. The mechanism by which COVID-infected patients develop cardiac complications remains unclear, though it may be mediated by increased ACE-2 gene expression. Despite initial concerns, there is no evidence that angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) therapy increases risk for myocardial injury among those infected with COVID-19. In the current report, we summarize the peer-reviewed and preprint literature on cardiovascular risks and complications associated with COVID-19, as well as provide insights into its pathogenesis and management.
Keywords: COVID-19; SARS-CoV-2; cardiovascular complications; cardiovascular risks; corona; coronavirus.
AJCD Copyright © 2020.
Conflict of interest statement
Dr. Krittanawong discloses the following relationships - Member of the American College of Cardiology Solution Set Oversight Committee, The Lancet Digital Health (Advisory Board), European Heart Journal Digital Health (Editorial board) and Journal of the American Heart Association (Editorial board). Dr. Virani discloses the following relationships: Grant from Department of Veterans Affairs, World Heart Federation, Jooma and Tahir Family. Honorarium: American College of Cardiology (Associate Editor for Innovations, acc.org). Steering Committee member: Patient and Provider Assessment of Lipid Management (PALM) registry at the Duke Clinical Research Institute (no. financial remuneration). Dr. Ballantyne discloses the following relationships: Grant/Research Support- All significant. (All paid to institution, not individual): Abbott Diagnostic, Akcea, Amgen, Esperion, Novartis, Regeneron, Roche Diagnostic, NIH, AHA, ADA. Consultant - Abbott Diagnostics, Akcea, Althera, Amarin*, Amgen, Arrowhead, Astra Zeneca, Corvidia, Denka Seiken*, Esperion, Gilead, Janssen, Matinas BioPharma Inc, New Amsterdam*, Novartis, Novo Nordisk, Pfizer, Regeneron, Roche Diagnostic, Sanofi-Synthelabo* [*Significant where noted (>$10,000); remainder modest (<$10,000)].
Figures
References
-
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506. - PMC - PubMed
-
- Martines RB, Ritter JM, Matkovic E, Gary J, Bollweg BC, Bullock H, Goldsmith CS, Silva-Flannery L, Seixas JN, Reagan-Steiner S, Uyeki T, Denison A, Bhatnagar J, Shieh WJ, Zaki SR. Pathology and pathogenesis of SARS-CoV-2 associated with fatal coronavirus disease, United States. Emerg Infect Dis. 2020;26:9. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous