

Molecular mechanisms of right ventricular dysfunction in pulmonary arterial hypertension: focus on the coronary vasculature, sex hormones, and glucose/lipid metabolism
- PMID: 33224772
- PMCID: PMC7666935
- DOI: 10.21037/cdt-20-404
Molecular mechanisms of right ventricular dysfunction in pulmonary arterial hypertension: focus on the coronary vasculature, sex hormones, and glucose/lipid metabolism
Abstract
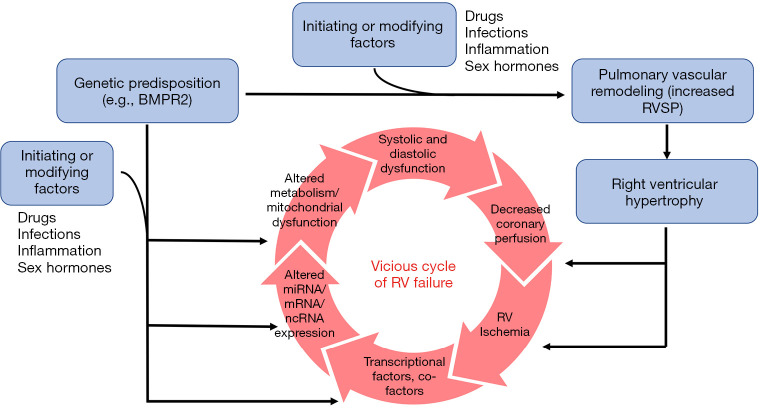
Pulmonary arterial hypertension (PAH) is a rare, life-threatening condition characterized by dysregulated metabolism, pulmonary vascular remodeling, and loss of pulmonary vascular cross-sectional area due to a variety of etiologies. Right ventricular (RV) dysfunction in PAH is a critical mediator of both long-term morbidity and mortality. While combinatory oral pharmacotherapy and/or intravenous prostacyclin aimed at decreasing pulmonary vascular resistance (PVR) have improved clinical outcomes, there are currently no treatments that directly address RV failure in PAH. This is, in part, due to the incomplete understanding of the pathogenesis of RV dysfunction in PAH. The purpose of this review is to discuss the current understanding of key molecular mechanisms that cause, contribute and/or sustain RV dysfunction, with a special focus on pathways that either have led to or have the potential to lead to clinical therapeutic intervention. Specifically, this review discusses the mechanisms by which vessel loss and dysfunctional angiogenesis, sex hormones, and metabolic derangements in PAH directly contribute to RV dysfunction. Finally, this review discusses limitations and future areas of investigation that may lead to novel understanding and therapeutic interventions for RV dysfunction in PAH.
Keywords: Pulmonary arterial hypertension (PAH); coronary vasculature; metabolism; right ventricular failure (RV failure); sex hormones.
2020 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/cdt-20-404). The series “Right Ventricular Dysfunction” was commissioned by the editorial office without any funding or sponsorship. GH served as the unpaid Guest Editors of the series. TL reports personal fees from Bayer, Inc., outside the submitted work. GH reports patent “Compositions and method for treatment of pulmonary hypertension”, 12/2009 USPTO application no. 1289344, Stanford University (Inventors: Georg Hansmann, Roham T. Zamanian, Marlene Rabinovitch). ARH reports personal fees from Actelion, personal fees from Bayer, personal fees from Complexa, personal fees from PHPrecisionMed, personal fees from united therapeutics, outside the submitted work. The author has no other conflicts of interest to declare.
Figures




References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials