

Mechanics of right ventricular dysfunction in pulmonary arterial hypertension and heart failure with preserved ejection fraction
- PMID: 33224775
- PMCID: PMC7666917
- DOI: 10.21037/cdt-20-479
Mechanics of right ventricular dysfunction in pulmonary arterial hypertension and heart failure with preserved ejection fraction
Abstract
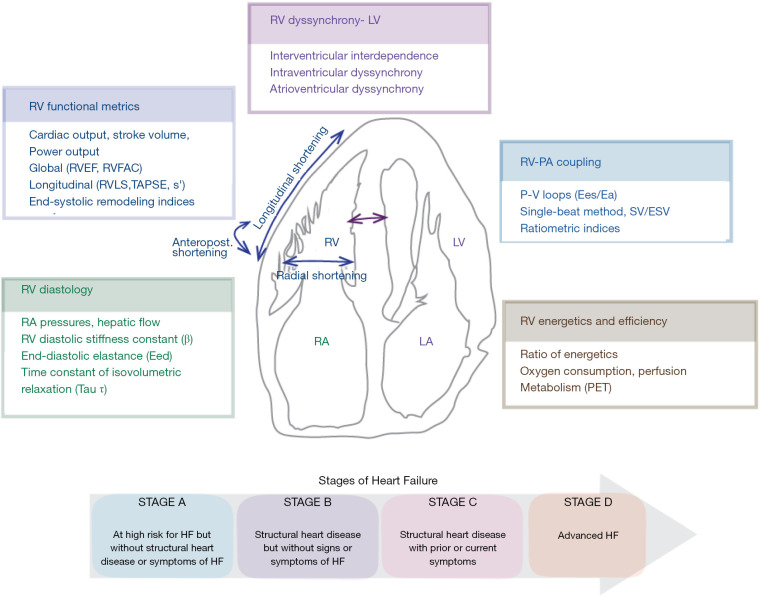
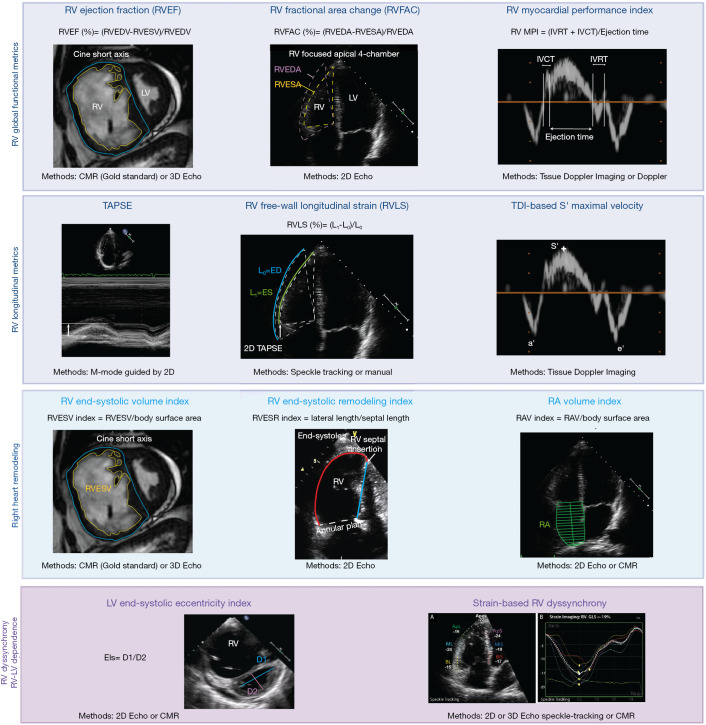
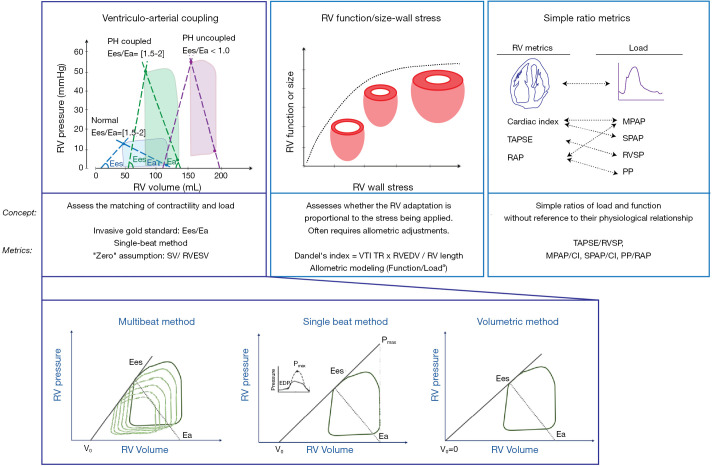
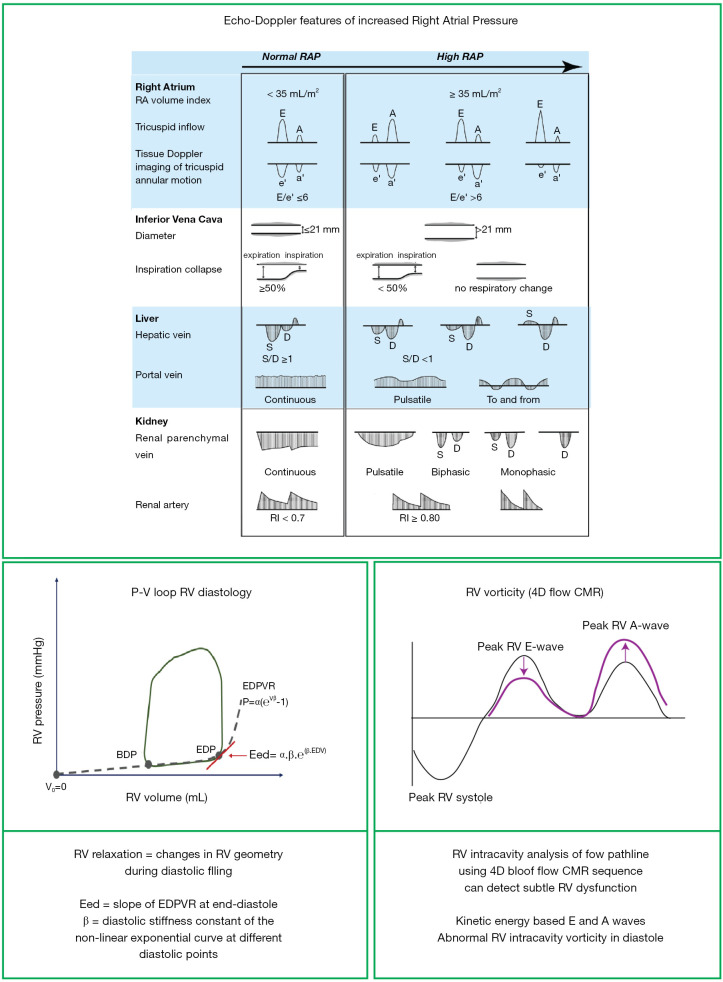
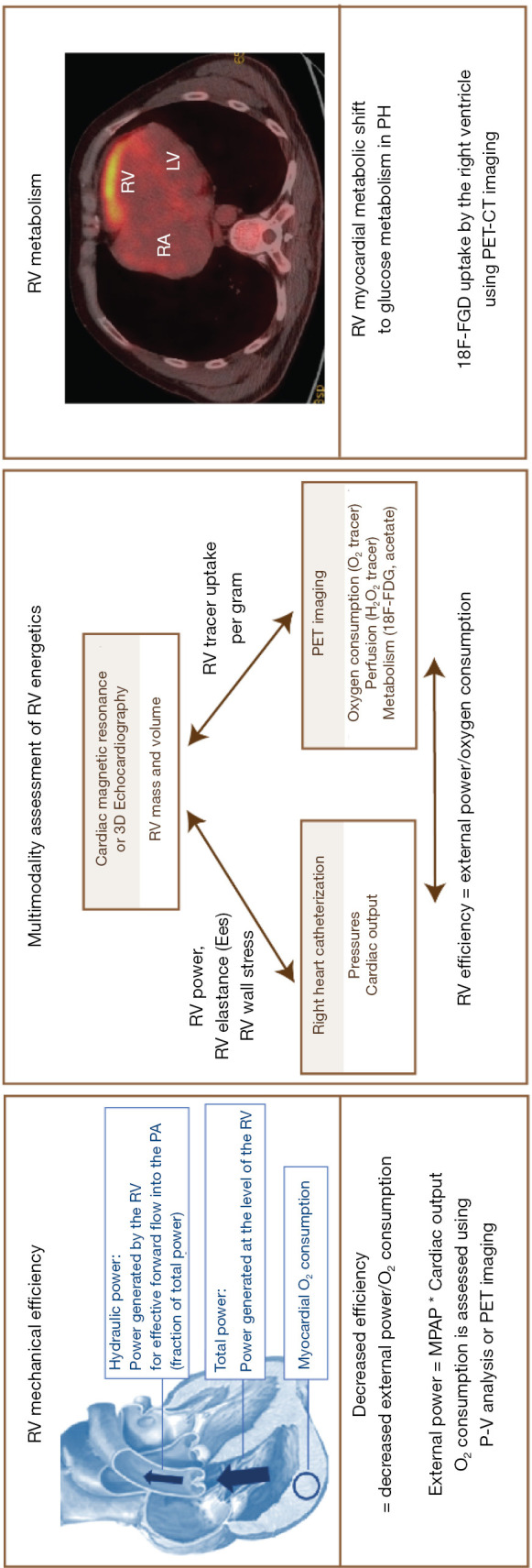
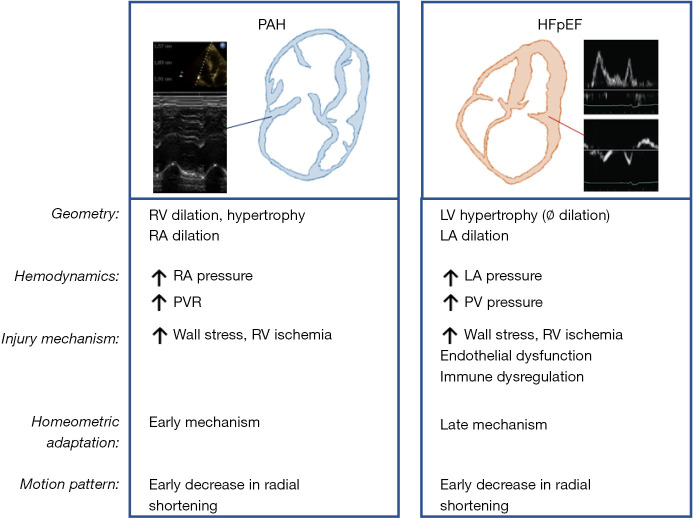
Right ventricular (RV) dysfunction is the most important determinant of survival in patients with pulmonary hypertension (PH). The manifestations of RV dysfunction not only include changes in global RV systolic function but also abnormalities in the pattern of contraction and synchrony. The effects of PH on the right ventricle have been mainly studied in patients with pulmonary arterial hypertension (PAH). However, with the demographic shift towards an aging population, heart failure with preserved ejection fraction (HFpEF) has become an important etiology of PH in recent years. There are significant differences in RV mechanics, function and adaptation between patients with PAH and HFpEF (with or without PH), which are related to different patterns of remodeling and dysfunction. Due to the unique features of the RV chamber, its connection with the main pulmonary artery and the pulmonary circulation, an understanding of the mechanics of RV function and its clinical significance is mandatory for both entities. In this review, we describe the mechanics of the pressure overloaded right ventricle. We review the different mechanical components of RV dysfunction and ventricular dyssynchrony, followed by insights via analysis of pressure-volume loop, energetics and novel blood flow patterns, such as vortex imaging. We conduct an in-depth comparison of prevalence and characteristics of RV dysfunction in HFpEF and PAH, and summarize key outcome studies. Finally, we provide a perspective on needed and expected future work in the field of RV mechanics.
Keywords: Heart failure with preserved ejection fraction (HFpEF); mechanical efficiency; pulmonary hypertension (PH); right ventricular dysfunction (RV dysfunction); ventriculo-arterial coupling.
2020 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/cdt-20-479). The series “Right Ventricular Dysfunction” was commissioned by the editorial office without any funding or sponsorship. GH served as the unpaid Guest Editor of the series. GH reports grants from German Research Foundation (DFG; HA4348/2-2 and HA4348/6-2 KFO311), from Federal Ministry of Education and Research (BMBF ViP+ program-03VP08053; BMBF 01KC2001B), from European Pediatric Pulmonary Vascular Disease Network (www.pvdnetwork.org), outside the submitted work. AYD reports grants from Edwards (2019) research (equipment grant), outside the submitted work; and Speaker bureau and KOL for CAE Healthcare and Masimo. Dr. FSdM reports grants from The Netherlands CardioVascular Research Initiative: the Dutch Heart Foundation, Dutch Federation of University Medical Centres, the Netherlands Organisation for Health Research and Development, and the Royal Netherlands Academy of Sciences (CVON-2012-08 PHAEDRA, CVON-2018-29 PHAEDRA-IMPACT, CVON-2017-10 Dolphin-Genesis), from The Netherlands Organization for Scientific Research (NWO-VIDI: 917.18.338), from The Dutch Heart Foundation Dekker senior post-doc grant (2018T059), outside the submitted work. The authors have no other conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources