

Development and Verification of a Digital Twin Patient Model to Predict Specific Treatment Response During the First 24 Hours of Sepsis
- PMID: 33225302
- PMCID: PMC7671877
- DOI: 10.1097/CCE.0000000000000249
Development and Verification of a Digital Twin Patient Model to Predict Specific Treatment Response During the First 24 Hours of Sepsis
Abstract
To develop and verify a digital twin model of critically ill patient using the causal artificial intelligence approach to predict the response to specific treatment during the first 24 hours of sepsis.
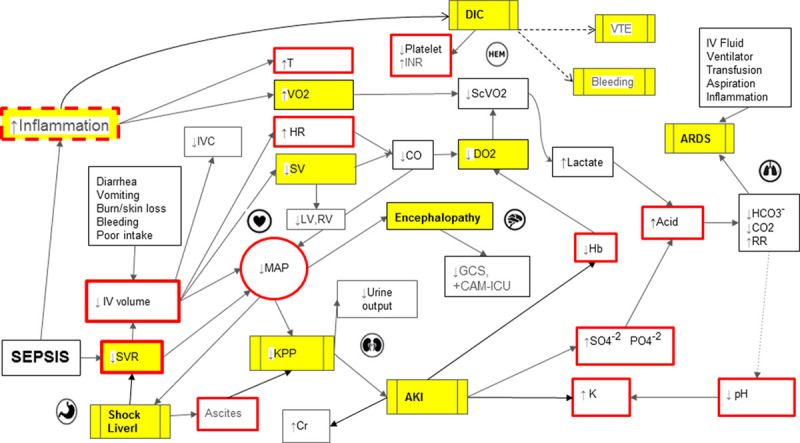
Design: Directed acyclic graphs were used to define explicitly the causal relationship among organ systems and specific treatments used. A hybrid approach of agent-based modeling, discrete-event simulation, and Bayesian network was used to simulate treatment effect across multiple stages and interactions of major organ systems (cardiovascular, neurologic, renal, respiratory, gastrointestinal, inflammatory, and hematology). Organ systems were visualized using relevant clinical markers. The application was iteratively revised and debugged by clinical experts and engineers. Agreement statistics was used to test the performance of the model by comparing the observed patient response versus the expected response (primary and secondary) predicted by digital twin.
Setting: Medical ICU of a large quaternary- care academic medical center in the United States.
Patients or subjects: Adult (> 18 year yr old), medical ICU patients were included in the study.
Interventions: No additional interventions were made beyond the standard of care for this study.
Measurements and main results: During the verification phase, model performance was prospectively tested on 145 observations in a convenience sample of 29 patients. Median age was 60 years (54-66 d) with a median Sequential Organ Failure Assessment score of 9.5 (interquartile range, 5.0-14.0). The most common source of sepsis was pneumonia, followed by hepatobiliary. The observations were made during the first 24 hours of the ICU admission with one-step interventions, comparing the output in the digital twin with the real patient response. The agreement between the observed versus and the expected response ranged from fair (kappa coefficient of 0.41) for primary response to good (kappa coefficient of 0.65) for secondary response to the intervention. The most common error detected was coding error in 50 observations (35%), followed by expert rule error in 29 observations (20%) and timing error in seven observations (5%).
Conclusions: We confirmed the feasibility of development and prospective testing of causal artificial intelligence model to predict the response to treatment in early stages of critical illness. The availability of qualitative and quantitative data and a relatively short turnaround time makes the ICU an ideal environment for development and testing of digital twin patient models. An accurate digital twin model will allow the effect of an intervention to be tested in a virtual environment prior to use on real patients.
Keywords: artificial intelligence; critical care; digital twin; directed acyclic graph; organ failure.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Bledsoe BE. The golden hour: Fact or fiction? Emerg Med Serv. 2002; 31:105 - PubMed
-
- Reinhart K, Daniels R, Kissoon N, et al. Recognizing sepsis as a global health priority - a WHO resolution. N Engl J Med. 2017; 377:414–417 - PubMed
-
- Rivers E, Nguyen B, Havstad S, et al. ; Early Goal-Directed Therapy Collaborative Group. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001; 345:1368–1377 - PubMed
-
- National Patient Safety Agency: Safer Care for the Acutely Ill Patient: Learning From Serious Incidents: The Fifth Report From the Patient Safety Observatory. Great Britain: National Patient Safety Agency, 2007
LinkOut - more resources
Full Text Sources
Other Literature Sources
