

Intravenous Immunoglobulin Plus Methylprednisolone Mitigate Respiratory Morbidity in Coronavirus Disease 2019
- PMID: 33225306
- PMCID: PMC7671875
- DOI: 10.1097/CCE.0000000000000280
Intravenous Immunoglobulin Plus Methylprednisolone Mitigate Respiratory Morbidity in Coronavirus Disease 2019
Abstract
Dysregulated neutrophil and platelet interactions mediate immunothrombosis and cause lung injury in coronavirus disease 2019. IV immunoglobulin modulates neutrophil activation through FcγRIII binding. We hypothesized that early therapy with IV immunoglobulin would abrogate immunothrombosis and improve oxygenation and reduce progression to mechanical ventilation in coronavirus disease 2019 pneumonia.
Design: Prospective randomized open label.
Setting: Inpatient hospital.
Patients and intervention: Hypoxic subjects with coronavirus disease 2019 pneumonia were randomized 1:1 to receive standard of care plus IV immunoglobulin 0.5 g/kg/d with methylprednisolone 40 mg 30 minutes before infusion for 3 days versus standard of care alone.
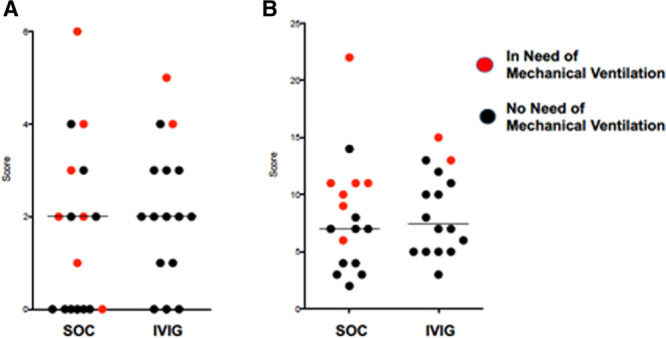
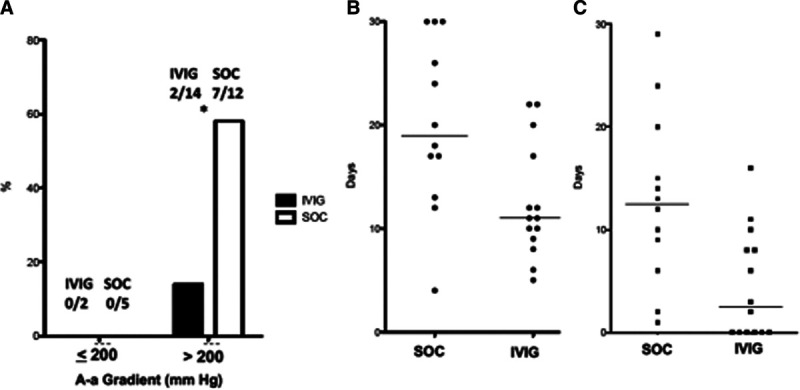
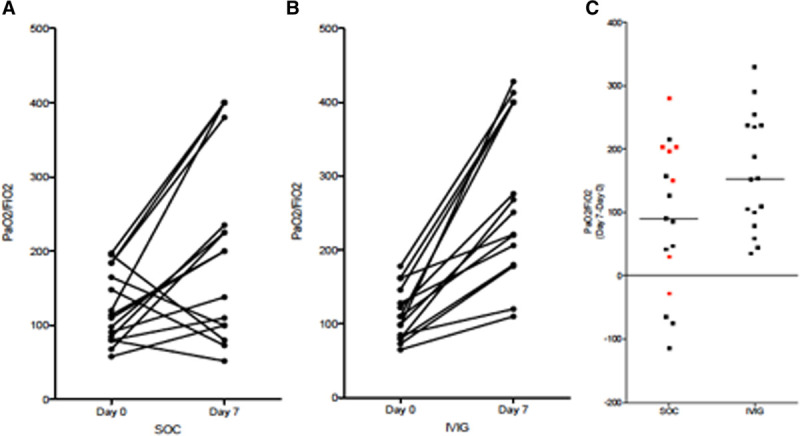
Main results: Sixteen subjects received IV immunoglobulin and 17 standard of care. Median ages were 51 and 58 years for standard of care and IV immunoglobulin, respectively. Acute Physiology and Chronic Health Evaluation II and Charlson comorbidity scores were similar for IV immunoglobulin and standard of care. Seven standard of care versus two IV immunoglobulin subjects required mechanical ventilation (p = 0.12, Fisher exact test). Among subjects with A-a gradient of greater than 200 mm Hg at enrollment, the IV immunoglobulin group showed: 1) a lower rate of progression to requiring mechanical ventilation (2/14 vs 7/12, p = 0.038 Fisher exact test), 2) shorter median hospital length of stay (11 vs 19 d, p = 0.01 Mann Whitney U test), 3) shorter median ICU stay (2.5 vs 12.5 d, p = 0.006 Mann Whitey U test), and 4) greater improvement in Pao2/Fio2 at 7 days (median [range] change from time of enrollment +131 [+35 to +330] vs +44·5 [-115 to +157], p = 0.01, Mann Whitney U test) than standard of care. Pao2/Fio2 improvement at day 7 was significantly less for the standard of care patients who received glucocorticoid therapy than those in the IV immunoglobulin arm (p = 0.0057, Mann Whiney U test).
Conclusions: This pilot study showed that IV immunoglobulin significantly improved hypoxia and reduced hospital length of stay and progression to mechanical ventilation in coronavirus disease 2019 patients with A-a gradient greater than 200 mm Hg. A phase 3 multicenter randomized double-blinded clinical trial is under way to validate these findings.
Keywords: coronavirus disease 2019; immunothrombosis; intravenous immunoglobulin; pneumonia.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Figures
References
-
- Galeotti C, Kaveri SV, Bayry J. IVIG-mediated effector functions in autoimmune and inflammatory diseases. Int Immunol. 2017; 29:491–498 - PubMed
LinkOut - more resources
Full Text Sources
