

Insufficient tuberculosis treatment leads to earlier and higher mortality in individuals co-infected with HIV in southern China: a cohort study
- PMID: 33225919
- PMCID: PMC7682080
- DOI: 10.1186/s12879-020-05527-0
Insufficient tuberculosis treatment leads to earlier and higher mortality in individuals co-infected with HIV in southern China: a cohort study
Abstract
Background: Tuberculosis (TB) and Acquired Immune Deficiency Syndrome (AIDS) are leading causes of death globally. However, little is known about the long-term mortality risk and the timeline of death in those co-infected with human immunodeficiency virus (HIV) and Mycobacterium tuberculosis (MTB). This study sought to understand the long-term mortality risk, factors, and the timeline of death in those with HIV-Mycobacterium tuberculosis (MTB) coinfection, particularly in those with insufficient TB treatment.
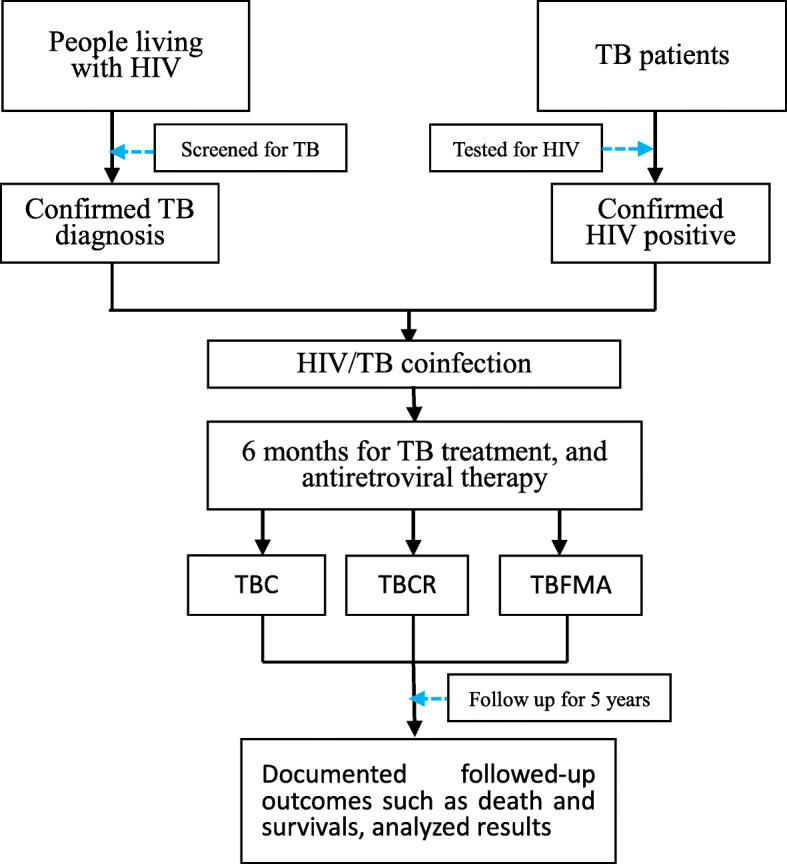
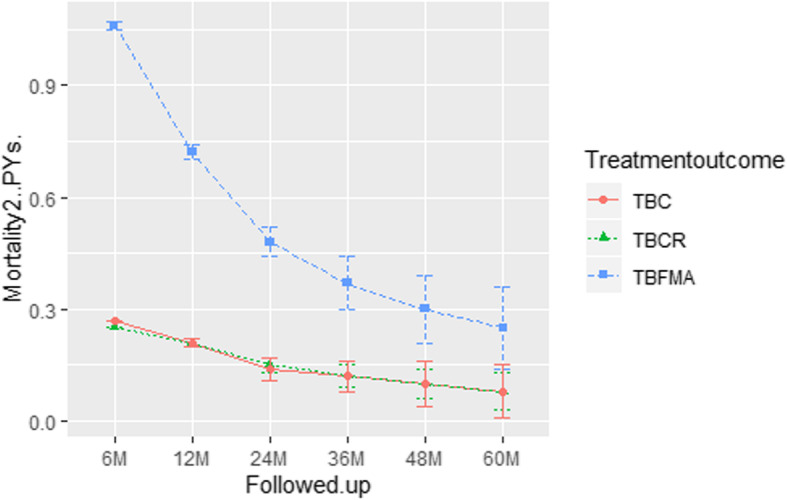
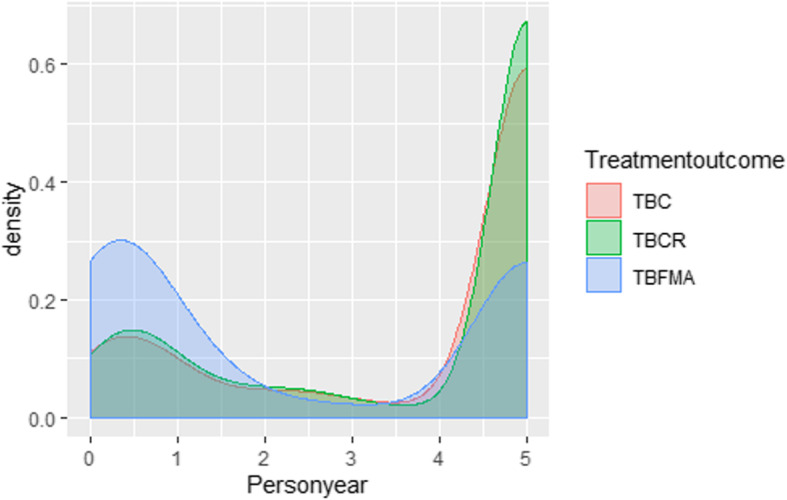
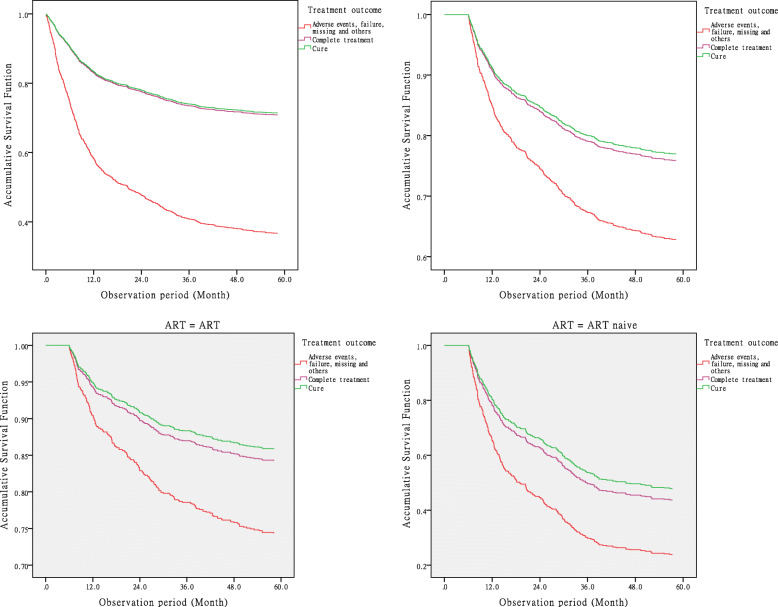
Methods: TB-cause specific deaths were classified using a modified 'Coding of Cause of Death in HIV' protocol. A longitudinal cross-registration-system checking approach was used to confirm HIV/MTB co-infection between two observational cohorts. Mortality from the end of TB treatment (6 months) to post-treatment year (PTY) 5 (60 months) was investigated by different TB treatment outcomes. General linear models were used to estimate the mean mortality at each time-point and change between time-points. Cox's proportional hazard regressions measured the mortality hazard risk (HR) at each time-point. The Mantel-Haenszel stratification was used to identify mortality risk factors. Mortality density was calculated by person year of follow-up.
Results: At the end point, mortality among patients with HIV/MTB coinfection was 34.7%. From the end of TB treatment to PTY5, mortality and loss of person years among individuals with TB treatment failure, missing, and adverse events (TBFMA) were significantly higher than those who had TB cure (TBC) and TB complete regimen (TBCR). Compared to individuals with TBC and with TBCR, individuals with TBFMA tended to die earlier and their mortality was significantly higher (HRTBFMA-TBC = 3.0, 95% confidence interval: 2.5-3.6, HRTBFMA-TBCR = 2.9, 95% CI: 2.5-3.4, P < 0.0001). Those who were naïve to antiretroviral therapy, were farmers, had lower CD4 counts (≤200 cells/μL) and were ≥ 50 years of age were at the highest risk of mortality. Mortality risk for participants with TBFMA was significantly higher across all stratifications except those with a CD4 count of ≤200 cells/μL.
Conclusions: Earlier and long-term mortality among those with HIV/MTB co-infection is a significant problem when TB treatment fails or is inadequate.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
[Impact of HIV and Mycobacterium tuberculosis co-infection on related mortality].Zhonghua Liu Xing Bing Xue Za Zhi. 2018 Oct 10;39(10):1362-1367. doi: 10.3760/cma.j.issn.0254-6450.2018.10.014. Zhonghua Liu Xing Bing Xue Za Zhi. 2018. PMID: 30453438 Chinese.
-
Chest X-ray interpretation does not complement Xpert MTB/RIF in diagnosis of smear-negative pulmonary tuberculosis among TB-HIV co-infected adults in a resource-limited setting.BMC Infect Dis. 2021 Jan 13;21(1):63. doi: 10.1186/s12879-020-05752-7. BMC Infect Dis. 2021. PMID: 33435896 Free PMC article.
-
Mortality risk in the population of HIV-positive individuals in Southern China: A cohort study.PLoS One. 2019 Feb 11;14(2):e0210856. doi: 10.1371/journal.pone.0210856. eCollection 2019. PLoS One. 2019. PMID: 30742626 Free PMC article. Clinical Trial.
-
Tuberculosis associated mortality in a prospective cohort in Sub Saharan Africa: Association with HIV and antiretroviral therapy.Int J Infect Dis. 2017 Mar;56:39-44. doi: 10.1016/j.ijid.2017.01.023. Epub 2017 Feb 1. Int J Infect Dis. 2017. PMID: 28161460 Review.
-
Novel developments in the epidemic of human immunodeficiency virus and tuberculosis coinfection.Am J Respir Crit Care Med. 2011 Apr 15;183(8):987-97. doi: 10.1164/rccm.201008-1246CI. Epub 2010 Dec 22. Am J Respir Crit Care Med. 2011. PMID: 21177884 Free PMC article. Review.
Cited by
-
Medical Care for Tuberculosis-HIV-Coinfected Patients in Russia with Respect to a Changeable Patients' Structure.Trop Med Infect Dis. 2022 May 31;7(6):86. doi: 10.3390/tropicalmed7060086. Trop Med Infect Dis. 2022. PMID: 35736965 Free PMC article.
-
Time trends in tuberculosis mortality across the BRICS: an age-period-cohort analysis for the GBD 2019.EClinicalMedicine. 2022 Sep 17;53:101646. doi: 10.1016/j.eclinm.2022.101646. eCollection 2022 Nov. EClinicalMedicine. 2022. PMID: 36147625 Free PMC article.
-
Diagnosis and Treatment of Skipped Multifocal Spinal Tuberculosis Lesions.Orthop Surg. 2023 Jun;15(6):1454-1467. doi: 10.1111/os.13744. Epub 2023 Apr 25. Orthop Surg. 2023. PMID: 37186216 Free PMC article. Review.
-
Treatment outcome and its associated factors among HIV-MTB co-infected patients in Sichuan, China: A retrospective study.Medicine (Baltimore). 2022 Dec 2;101(48):e32006. doi: 10.1097/MD.0000000000032006. Medicine (Baltimore). 2022. PMID: 36482608 Free PMC article.
-
Burden of mortality and its predictors among TB-HIV co-infected patients in Ethiopia: Systematic review and meta-analysis.PLoS One. 2024 Nov 7;19(11):e0312698. doi: 10.1371/journal.pone.0312698. eCollection 2024. PLoS One. 2024. PMID: 39509354 Free PMC article.
References
-
- World Health Organization . Global tuberculosis report 2017. Geneva: World Health Organization; 2017.
-
- World Health Organization . Global tuberculosis report 2015. Geneva: World Health Organization; 2015.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
