

Kidney biopsy findings in two patients with TAFRO syndrome: case presentations and review of the literature
- PMID: 33225930
- PMCID: PMC7682079
- DOI: 10.1186/s12882-020-02119-7
Kidney biopsy findings in two patients with TAFRO syndrome: case presentations and review of the literature
Abstract
Background: TAFRO syndrome is a clinical subtype of idiopathic multicentric Castleman disease (iMCD) that is characterized by thrombocytopenia, anasarca, fever, reticulin myelofibrosis (or renal dysfunction), and organomegaly. TAFRO syndrome has only recently been described, and many clinicians are unaware of this disease, leading to delays in diagnosis and treatment. We present two patients with TAFRO syndrome in whom renal biopsies were performed.
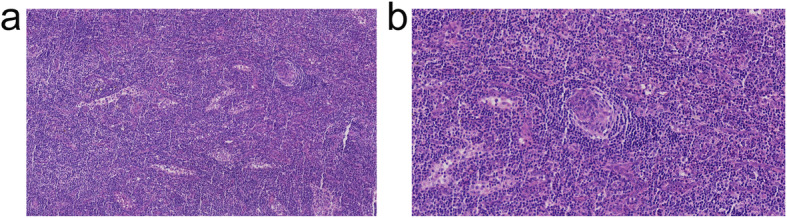
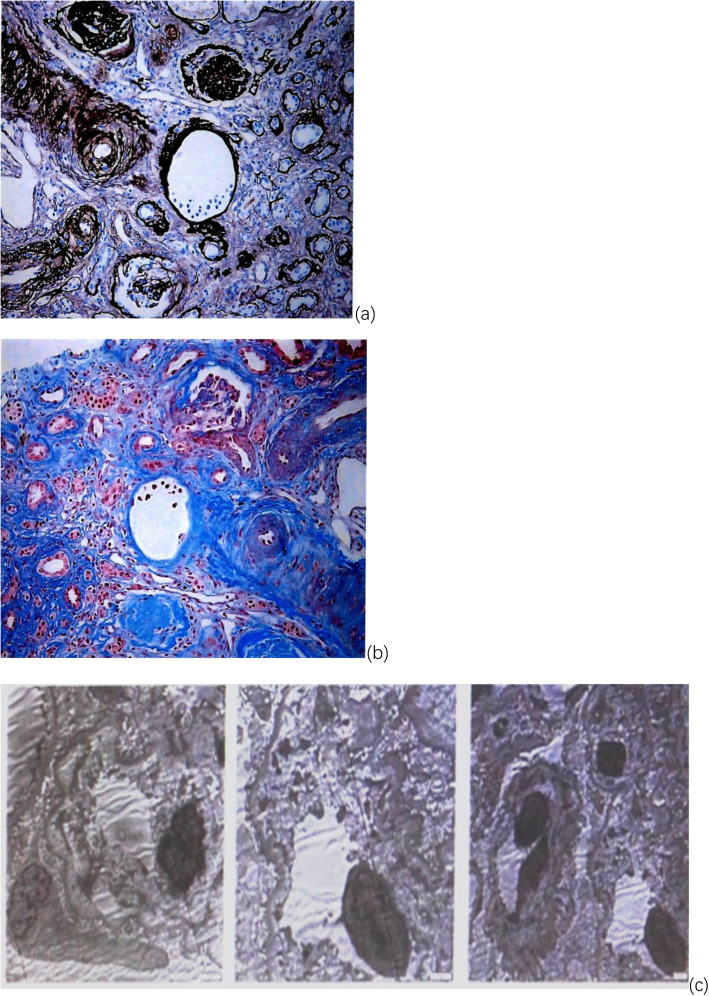
Case presentation: Both patients had subacute onset and exhibited renal insufficiency, edema, anemia, thrombocytopenia, polyserositis and lymphadenopathy over the disease course. However, there were many differences in their clinical manifestations. Case 1 was a 30-year-old woman admitted due to intermittent vaginal bleeding for 3 weeks. Laboratory tests on admission showed severe renal insufficiency (creatinine: 624 μmol/L), severe anemia (Hb: 41 g/L), and moderate thrombocytopenia (61 × 109/L). Case 2 was a 42-year-old man. Acute epigastric pain was his initial complaint, and computed tomography (CT) revealed retroperitoneal exudation around the pancreas. He was diagnosed with acute pancreatitis, and after treatment with a proton pump inhibitor (PPI) and somatostatin, his abdominal pain still recurred. During treatment, renal failure gradually increased, with oliguria, fever, anemia, thrombocytopenia, edema and massive ascites. Lymph node histologies were consistent with the hyaline-vascular (HV) type and mixed type, respectively, and renal histopathologies were consistent with thrombotic microangiopathy (TMA)-like renal lesions and membranoproliferative glomerulonephritis (MPGN), respectively. Their general conditions improved after glucocorticoid therapy, but their renal functions did not recover completely. On the basis of glucocorticoids, second-line treatments with tocilizumab and rituximab, respectively, were applied.
Conclusions: The diagnosis of TAFRO syndrome is based mainly on clinical manifestations and lymph node biopsies. A reliable early diagnosis and appropriate rapid treatment are essential to improve patient outcomes. Clinicians should deepen their understanding of this disease and similar conditions. Once the disease is suspected, lymph node biopsies should be performed as soon as possible. In addition, renal biopsies should be actively performed in patients with renal involvement.
Keywords: Biopsy; Castleman disease; Kidney; Lymph node; Renal insufficiency; TAFRO syndrome.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures



References
-
- Flendrig JA, Schillings PHM. Benign giant lymphoma: the clinical signs and symptoms and the morphological aspects.y. Folia Med Neerl. 1969;12:119–120.
-
- Lachant NA, Sun NC, Leong LA, Oseas RS, Prince HE. Multicentric angiofollicular lymph node hyperplasia (Castleman’s disease) followed by Kaposi’s sarcoma in two homosexual males with the acquired immunodeficiency syndrome (AIDS) Am J Clin Pathol. 1985;83(1):27–33. doi: 10.1093/ajcp/83.1.27. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
