

Dosing of thromboprophylaxis and mortality in critically ill COVID-19 patients
- PMID: 33225952
- PMCID: PMC7680989
- DOI: 10.1186/s13054-020-03375-7
Dosing of thromboprophylaxis and mortality in critically ill COVID-19 patients
Abstract
Background: A substantial proportion of critically ill COVID-19 patients develop thromboembolic complications, but it is unclear whether higher doses of thromboprophylaxis are associated with lower mortality rates. The purpose of the study was to evaluate the association between initial dosing strategy of thromboprophylaxis in critically ill COVID-19 patients and the risk of death, thromboembolism, and bleeding.
Method: In this retrospective study, all critically ill COVID-19 patients admitted to two intensive care units in March and April 2020 were eligible. Patients were categorized into three groups according to initial daily dose of thromboprophylaxis: low (2500-4500 IU tinzaparin or 2500-5000 IU dalteparin), medium (> 4500 IU but < 175 IU/kilogram, kg, of body weight tinzaparin or > 5000 IU but < 200 IU/kg of body weight dalteparin), and high dose (≥ 175 IU/kg of body weight tinzaparin or ≥ 200 IU/kg of body weight dalteparin). Thromboprophylaxis dosage was based on local standardized recommendations, not on degree of critical illness or risk of thrombosis. Cox proportional hazards regression was used to estimate hazard ratios with corresponding 95% confidence intervals of death within 28 days from ICU admission. Multivariable models were adjusted for sex, age, body mass index, Simplified Acute Physiology Score III, invasive respiratory support, and initial dosing strategy of thromboprophylaxis.
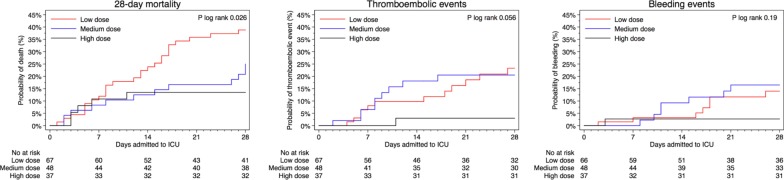
Results: A total of 152 patients were included: 67 received low-, 48 medium-, and 37 high-dose thromboprophylaxis. Baseline characteristics did not differ between groups. For patients who received high-dose prophylaxis, mortality was lower (13.5%) compared to those who received medium dose (25.0%) or low dose (38.8%), p = 0.02. The hazard ratio of death was 0.33 (95% confidence intervals 0.13-0.87) among those who received high dose, and 0.88 (95% confidence intervals 0.43-1.83) among those who received medium dose, as compared to those who received low-dose thromboprophylaxis. There were fewer thromboembolic events in the high (2.7%) vs medium (18.8%) and low-dose thromboprophylaxis (17.9%) groups, p = 0.04.
Conclusions: Among critically ill COVID-19 patients with respiratory failure, high-dose thromboprophylaxis was associated with a lower risk of death and a lower cumulative incidence of thromboembolic events compared with lower doses.
Trial registration: Clinicaltrials.gov NCT04412304 June 2, 2020, retrospectively registered.
Keywords: Anticoagulation; COVID-19; Critical care; Low molecular weight heparin; SARS-CoV-2; Thromboembolism.
Conflict of interest statement
M. Cronhjort has honoraria for lectures from B. Braun. With this exception the authors declare that they have no competing interests.
Figures
References
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
