A National Study of Life-Sustaining Treatments in South Korea: What Factors Affect Decision-Making?
- PMID: 33227190
- PMCID: PMC8053857
- DOI: 10.4143/crt.2020.803
A National Study of Life-Sustaining Treatments in South Korea: What Factors Affect Decision-Making?
Abstract
Purpose: This cross-sectional study investigated the status of life-sustaining treatment (LST) practices and identified characteristics and factors influencing decision-making practices.
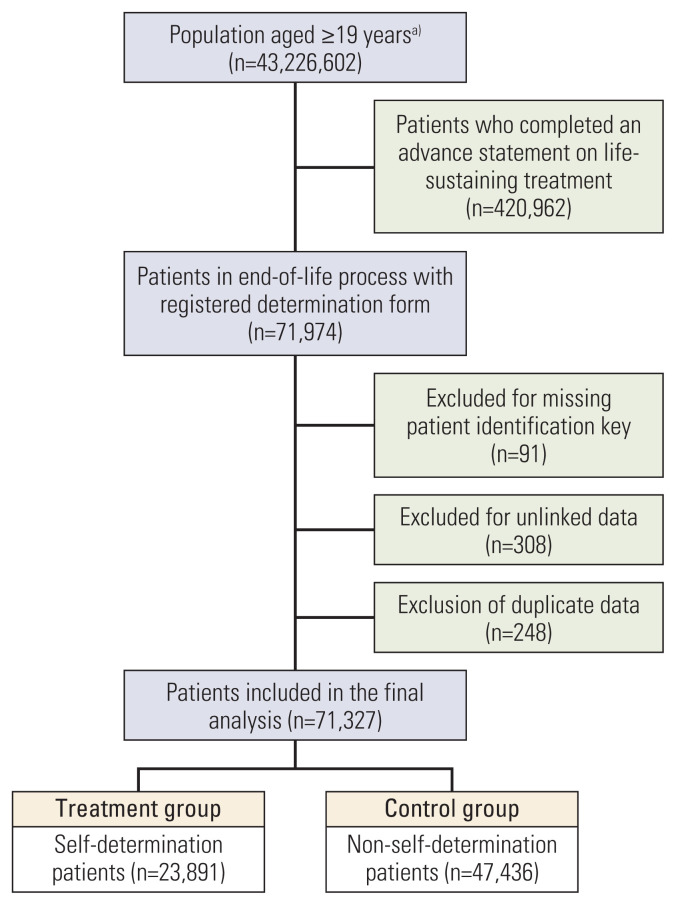
Materials and methods: The National Agency for Management of Life-sustaining Treatment retains records provided by doctors regarding patients subject to LST implementation. A total of 71,327 patients receiving LST were identified. We analyzed all nationally reported data between February 2018 and October 2019. Indicators such as the proportion of deaths, records for decision to terminate LST, implementation of LST records, and registration of Advance Statements on LST were analyzed.
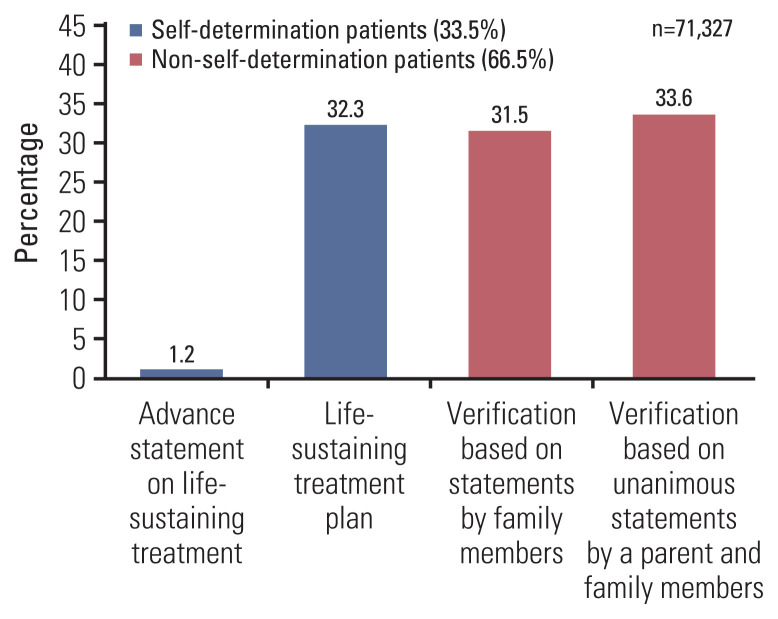
Results: A total of 67,252 (94.3%) end-of life decisions were implemented in South Korea. The proportion of deaths preceded by a LST plan, non-self-determination LST decision, and any advance statements was 33.5% (23,891/71,327), 66.5% (47,436/71,327), and 1.2% (890/71,327), respectively. The logistic regression model revealed that self-determination to terminate LST was more frequent for men than for women and higher for those aged 30-69. Disability (odds ratio [OR], 0.59; 95% confidence interval [CI], 0.56 to 0.61), living in non-metropolitan areas (OR, 0.84; 95% CI, 0.81 to 0.86), and disease comorbidity was independently associated with a low level of self-determination.
Conclusion: After the implementation of the new LST Act, about a third of patients in end-of-life process made decisions regarding their medical LST. However, family members still play a major role in LST decisions where the patient's intention cannot be verified. Decisions related to LST are predominantly made when death is imminent. Thus, it is necessary to increase awareness of end-of-life LST decision-making among medical staff and the public.
Keywords: Cross-sectional studies; Hospice; Medical staff; Palliative care; Personal autonomy; Terminal care.
Conflict of interest statement
Conflict of interest relevant to this article was not reported.
Figures
References
-
- Cook D, Rocker G, Marshall J, Sjokvist P, Dodek P, Griffith L, et al. Withdrawal of mechanical ventilation in anticipation of death in the intensive care unit. N Engl J Med. 2003;349:1123–32. - PubMed
-
- Yaguchi A, Truog RD, Curtis JR, Luce JM, Levy MM, Melot C, et al. International differences in end-of-life attitudes in the intensive care unit: results of a survey. Arch Intern Med. 2005;165:1970–5. - PubMed
-
- Phua J, Joynt GM, Nishimura M, Deng Y, Myatra SN, Chan YH, et al. Withholding and withdrawal of life-sustaining treatments in intensive care units in Asia. JAMA Intern Med. 2015;175:363–71. - PubMed
-
- Frost DW, Cook DJ, Heyland DK, Fowler RA. Patient and healthcare professional factors influencing end-of-life decision-making during critical illness: a systematic review. Crit Care Med. 2011;39:1174–89. - PubMed
-
- Crawley LM, Marshall PA, Lo B, Koenig BA End-of-Life Care Consensus Panel. Strategies for culturally effective end-of-life care. Ann Intern Med. 2002;136:673–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources