

Clinical trials in critical care: can a Bayesian approach enhance clinical and scientific decision making?
- PMID: 33227237
- PMCID: PMC8439199
- DOI: 10.1016/S2213-2600(20)30471-9
Clinical trials in critical care: can a Bayesian approach enhance clinical and scientific decision making?
Abstract
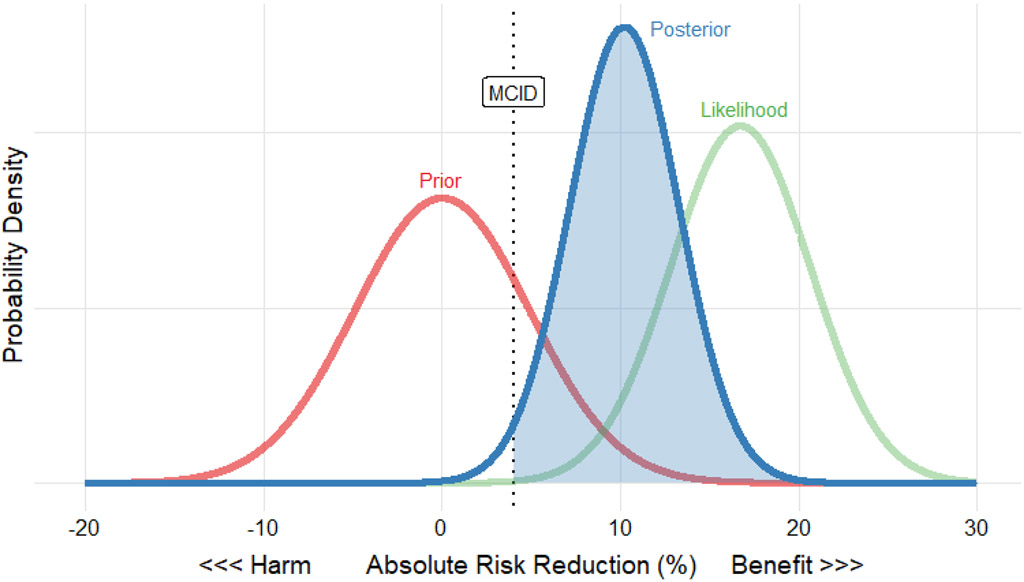
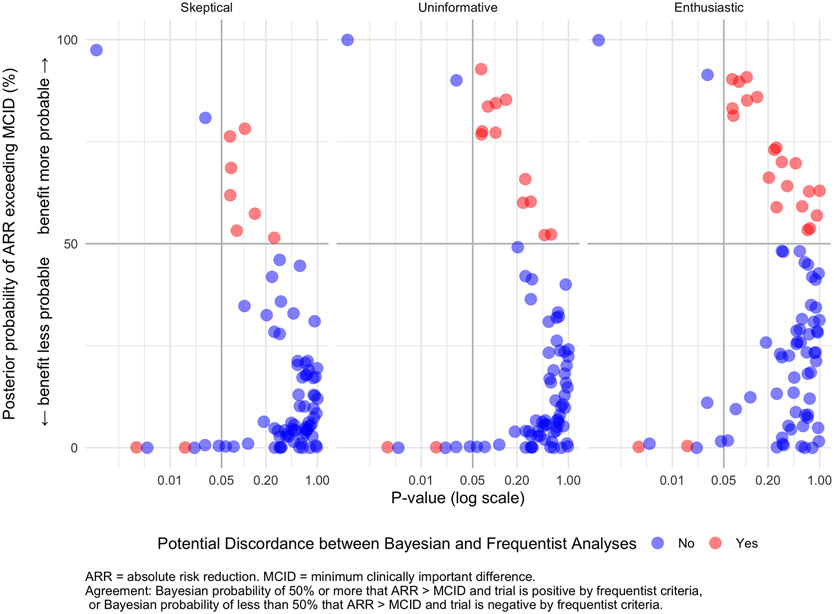
Recent Bayesian reanalyses of prominent trials in critical illness have generated controversy by contradicting the initial conclusions based on conventional frequentist analyses. Many clinicians might be sceptical that Bayesian analysis, a philosophical and statistical approach that combines prior beliefs with data to generate probabilities, provides more useful information about clinical trials than the frequentist approach. In this Personal View, we introduce clinicians to the rationale, process, and interpretation of Bayesian analysis through a systematic review and reanalysis of interventional trials in critical illness. In the majority of cases, Bayesian and frequentist analyses agreed. In the remainder, Bayesian analysis identified interventions where benefit was probable despite the absence of statistical significance, where interpretation depended substantially on choice of prior distribution, and where benefit was improbable despite statistical significance. Bayesian analysis in critical care medicine can help to distinguish harm from uncertainty and establish the probability of clinically important benefit for clinicians, policy makers, and patients.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declarations of interest
Dr. Brodie reports grants from ALung Technologies, personal fees from Baxter, personal fees from Xenios, personal fees from BREETHE, other from Hemovent, outside the submitted work. Dr. Beitler reports speaking fees from Hamilton Medical and consulting fees from Sedana Medical outside the scope of this work. Dr. Slutsky reports being on the medical advisory board for Baxter and for Novalung/Xenios, outside the scope of this work. Outside the submitted work, Dr. McAuley reports personal fees from consultancy for GlaxoSmithKline, Boehringer Ingelheim and Bayer. In addition, Dr. McAuley has a patent issued to his institution for a treatment for ARDS. DFM is a Director of Research for the Intensive Care Society and NIHR EME Programme Director. Dr. Goligher reports personal fees and non-financial support from Getinge, non-financial support from Timpel, outside the submitted work. Dr. Tomlinson reports personal fees from Spectral Medical Inc., outside the submitted work. Dr. Ferguson reports personal fees from XENIOS, personal fees from GETINGE, outside the submitted work. Dr. Fan reports personal fees from ALung Technologies, personal fees from Fresenius Medical Care, personal fees from MC3 Cardiopulmonary, outside the submitted work. All other authors declare no conflicts of interest.
Figures
Similar articles
-
A Bayesian approach to stochastic cost-effectiveness analysis.Health Econ. 1999 May;8(3):257-61. doi: 10.1002/(sici)1099-1050(199905)8:3<257::aid-hec427>3.0.co;2-e. Health Econ. 1999. PMID: 10348420
-
Bayesian methodology for the design and interpretation of clinical trials in critical care medicine: a primer for clinicians.Crit Care Med. 2014 Oct;42(10):2267-77. doi: 10.1097/CCM.0000000000000576. Crit Care Med. 2014. PMID: 25226118
-
Bayesian statistics for clinical research.Lancet. 2024 Sep 14;404(10457):1067-1076. doi: 10.1016/S0140-6736(24)01295-9. Lancet. 2024. PMID: 39277290 Free PMC article. Review.
-
Heterogeneity, Bayesian thinking, and phenotyping in critical care: A primer.Am J Health Syst Pharm. 2024 Sep 9;81(18):812-832. doi: 10.1093/ajhp/zxae139. Am J Health Syst Pharm. 2024. PMID: 38742459 Review.
-
Statistical primer: an introduction into the principles of Bayesian statistical analyses in clinical trials.Eur J Cardiothorac Surg. 2025 Mar 28;67(4):ezaf139. doi: 10.1093/ejcts/ezaf139. Eur J Cardiothorac Surg. 2025. PMID: 40221858 Free PMC article.
Cited by
-
Bayes and the Evidence Base: Reanalyzing Trials Using Many Priors Does Not Contribute to Consensus.Am J Respir Crit Care Med. 2024 Mar 1;209(5):483-484. doi: 10.1164/rccm.202308-1455VP. Am J Respir Crit Care Med. 2024. PMID: 37922492 Free PMC article. No abstract available.
-
Non-inferiority and clinical superiority of glucagon-like peptide-1 receptor agonists and sodium-glucose co-transporter-2 inhibitors: Systematic analysis of cardiorenal outcome trials in type 2 diabetes.Diabetes Obes Metab. 2022 Aug;24(8):1598-1606. doi: 10.1111/dom.14735. Epub 2022 May 29. Diabetes Obes Metab. 2022. PMID: 35491523 Free PMC article.
-
Focused Ultrasound Neuromodulation: Exploring a Novel Treatment for Severe Opioid Use Disorder.Biol Psychiatry. 2025 Jul 1;98(1):56-64. doi: 10.1016/j.biopsych.2025.01.001. Epub 2025 Jan 9. Biol Psychiatry. 2025. PMID: 39798597
-
Between-trial heterogeneity in ARDS research.Intensive Care Med. 2021 Apr;47(4):422-434. doi: 10.1007/s00134-021-06370-w. Epub 2021 Mar 13. Intensive Care Med. 2021. PMID: 33713156 Free PMC article.
-
Bayesian methods: a potential path forward for sepsis trials.Crit Care. 2023 Nov 8;27(1):432. doi: 10.1186/s13054-023-04717-x. Crit Care. 2023. PMID: 37940985 Free PMC article.
References
-
- Greenland S Statistical tests, P values, confidence intervals, and power: a guide to misinterpretations. Eur J Epidemiol. 2016;31(4). http://resolver.scholarsportal.info/resolve/03932990/v31i0004/337_stpvci....Accessed June 6, 2019. - PMC - PubMed
-
- Wasserstein RL, Lazar NA. The ASA’s Statement on p -Values: Context, Process, and Purpose. Am Stat. 2016;70(2):129–133. doi:10.1080/00031305.2016.1154108 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
