

Clinical Impact of a Dedicated Trauma Hybrid Operating Room
- PMID: 33227422
- PMCID: PMC8005485
- DOI: 10.1016/j.jamcollsurg.2020.11.008
Clinical Impact of a Dedicated Trauma Hybrid Operating Room
Abstract
Background: Early hemorrhage control is essential to optimal trauma care. Hybrid operating rooms offer early, concomitant performance of advanced angiographic and operative hemostasis techniques, but their clinical impact is unclear. Herein, we present our initial experience with a dedicated, trauma hybrid operating room.
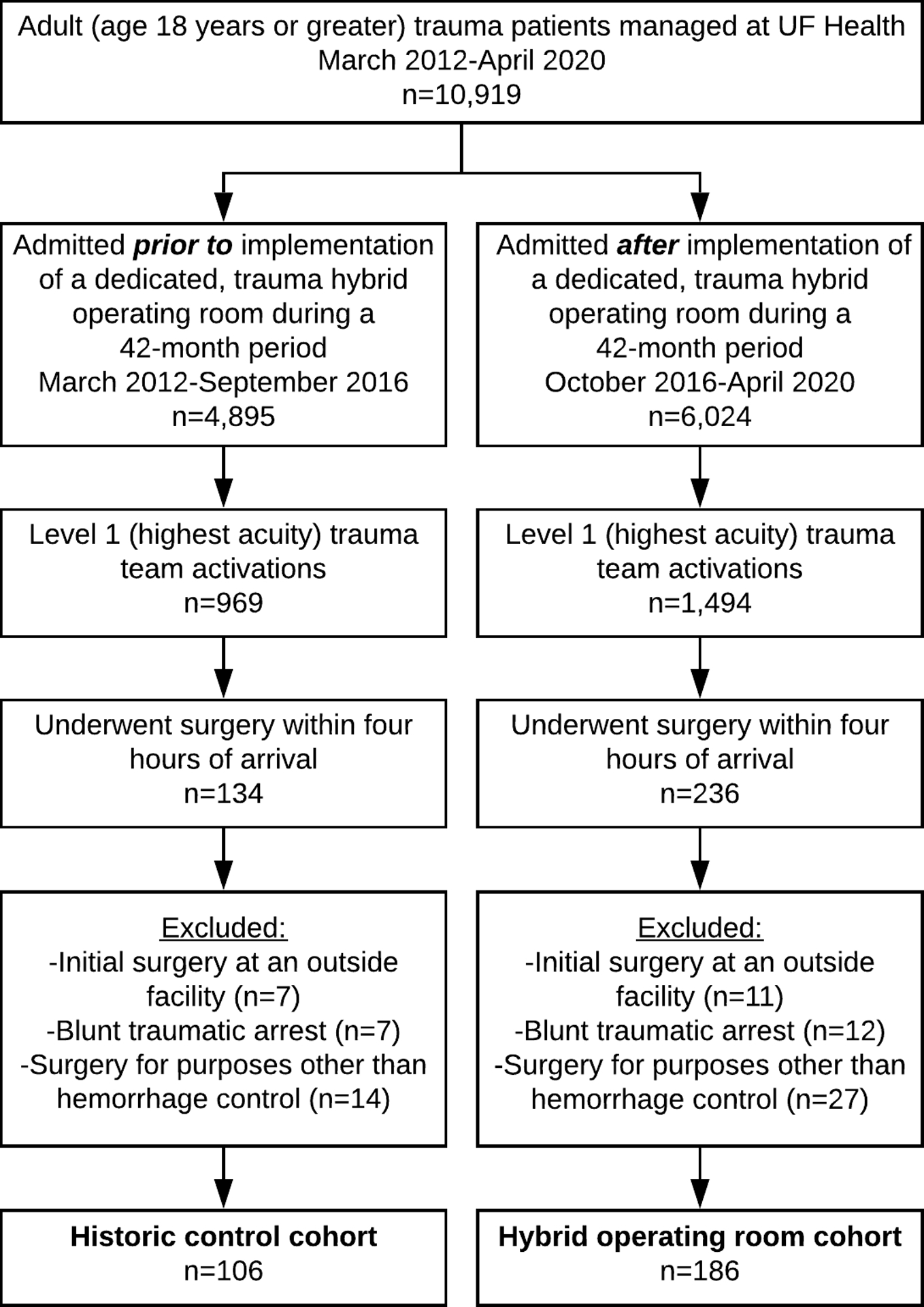
Study design: This retrospective cohort analysis of 292 adult trauma patients undergoing immediate surgery at a Level I trauma center compared patients managed after implementation of a dedicated, trauma hybrid operating room (n = 186) with historic controls (n = 106). The primary outcomes were time to hemorrhage control (systolic blood pressure ≥ 100 mmHg without ongoing vasopressor or transfusion requirements), early blood product administration, and complication.
Results: Patient characteristics were similar between cohorts (age 41 years, 25% female, 38% penetrating trauma). The hybrid cohort had lower initial hemoglobin (10.2 vs 11.1 g/dL, p = 0.001) and a greater proportion of patients undergoing resuscitative endovascular balloon occlusion of the aorta (9% vs 1%, p = 0.007). Cohorts had similar case mixes and intraoperative consultation with cardiothoracic or vascular surgery (13%). Twenty-one percent of all hybrid cases included angiography. The interval between operating room arrival and hemorrhage control was shorter in the hybrid cohort (49 vs 60 minutes, p = 0.005). From 4 to 24 hours after arrival, the hybrid cohort had fewer red cell (0.0 vs 1.0, p = 0.001) and plasma transfusions (0.0 vs 1.0, p < 0.001). The hybrid cohort had fewer infectious complications (15% vs 27%, p = 0.009) and ventilator days (2.0 vs 3.0, p = 0.011), and similar in-hospital mortality (13% vs 10%, p = 0.579).
Conclusions: Implementation of a dedicated, trauma hybrid operating room was associated with earlier hemorrhage control and fewer early blood transfusions, infectious complications, and ventilator days.
Copyright © 2020. Published by Elsevier Inc.
Figures

Comment in
-
Invited Commentary.J Am Coll Surg. 2021 Apr;232(4):570-571. doi: 10.1016/j.jamcollsurg.2020.12.047. J Am Coll Surg. 2021. PMID: 33771314 No abstract available.
-
Dedicated Trauma Hybrid Operating Room: Let Us Go Further.J Am Coll Surg. 2022 Jun 1;234(6):1255-1256. doi: 10.1097/XCS.0000000000000153. Epub 2022 Feb 22. J Am Coll Surg. 2022. PMID: 35703825 No abstract available.
References
-
- Peden M, McGee K, Sharma G. The injury chart book: a graphical overview of the global burden of injuries. Geneva: World Health Organization. 2002;5.
-
- Years of Potential Life Lost (YPLL) Reports, 1999 – 2015. Available at: https://webappa.cdc.gov/sasweb/ncipc/ypll10.html. Acessed June 9, 2020.
-
- Sauaia A, Moore FA, Moore EE, et al. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38(2):185–193. - PubMed
-
- Hoyt DB, Bulger EM, Knudson MM, et al. Death in the operating room: an analysis of a multi-center experience. J Trauma. 1994;37(3):426–432. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
