

Poverty and Targeted Immunotherapy: Survival in Children's Oncology Group Clinical Trials for High-Risk Neuroblastoma
- PMID: 33227816
- PMCID: PMC7936051
- DOI: 10.1093/jnci/djaa107
Poverty and Targeted Immunotherapy: Survival in Children's Oncology Group Clinical Trials for High-Risk Neuroblastoma
Abstract
Background: Whether social determinants of health are associated with survival in the context of pediatric oncology-targeted immunotherapy trials is not known. We examined the association between poverty and event-free survival (EFS) and overall survival (OS) for children with high-risk neuroblastoma treated in targeted immunotherapy trials.
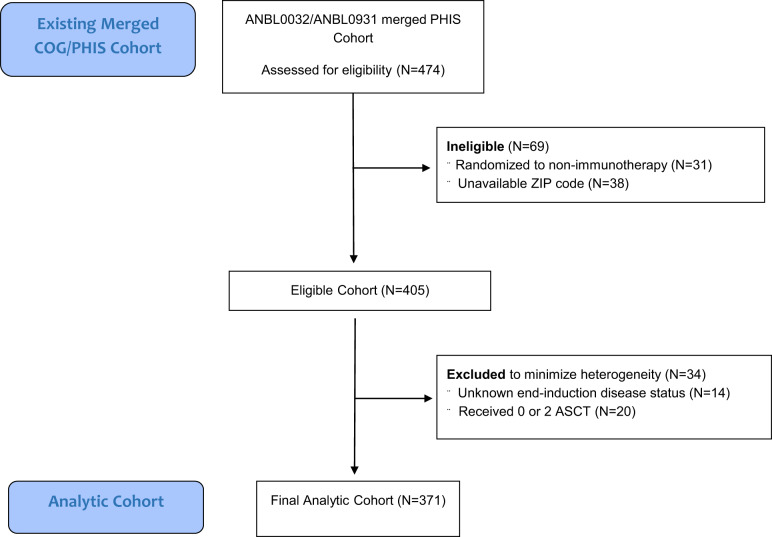
Methods: We conducted a retrospective cohort study of 371 children with high-risk neuroblastoma treated with GD2-targeted immunotherapy in the Children's Oncology Group trial ANBL0032 or ANBL0931 at a Pediatric Health Information System center from 2005 to 2014. Neighborhood poverty exposure was characterized a priori as living in a zip code with a median household income within the lowest quartile for the cohort. Household poverty exposure was characterized a priori as sole coverage by public insurance. Post hoc analyses examined the joint effect of neighborhood and household poverty using a common reference. All statistical tests were 2-sided.
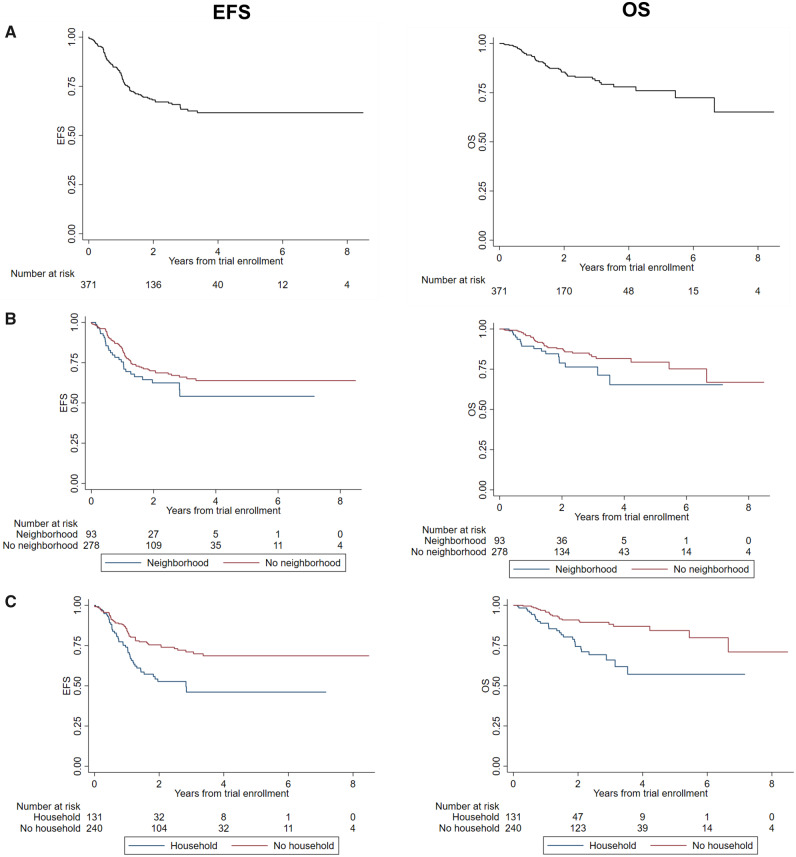
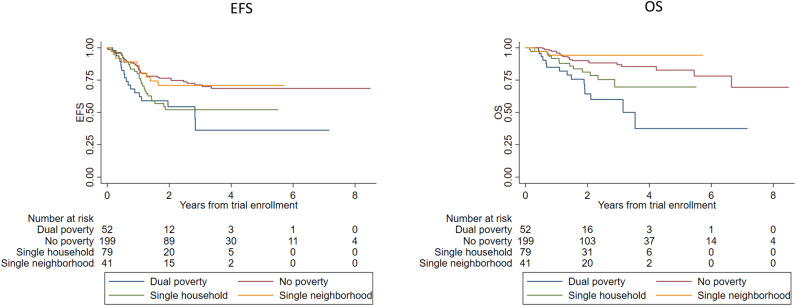
Results: In multivariable Cox regressions adjusted for disease and treatment factors, household poverty-exposed children experienced statistically significantly inferior EFS (hazard ratio [HR] = 1.90, 95% confidence interval [CI] = 1.28 to 2.82, P = .001) and OS (HR = 2.79, 95% CI = 1.63 to 4.79, P < .001) compared with unexposed children. Neighborhood poverty was not independently associated with EFS or OS. In post hoc analyses exploring the joint effect of neighborhood and household poverty, children with dual-poverty exposure (neighborhood poverty and household poverty) experienced statistically significantly inferior EFS (HR = 2.21, 95% CI = 1.48 to 3.30, P < .001) and OS (HR = 3.70, 95% CI = 2.08 to 6.59, P < .001) compared with the unexposed group.
Conclusions: Poverty is independently associated with increased risk of relapse and death among neuroblastoma patients treated with targeted immunotherapy. Incorporation of social and environmental factors in future trials as health-care delivery intervention targets may increase the benefit of targeted therapies.
© The Author(s) 2020. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Poverty and Survival in Childhood Cancer: A Framework to Move Toward Systemic Change.J Natl Cancer Inst. 2021 Mar 1;113(3):227-230. doi: 10.1093/jnci/djaa108. J Natl Cancer Inst. 2021. PMID: 33227815 Free PMC article. No abstract available.
