

Procalcitonin to Reduce Antibiotic Exposure during Acute Chest Syndrome in Adult Patients with Sickle-Cell Disease
- PMID: 33228148
- PMCID: PMC7699579
- DOI: 10.3390/jcm9113718
Procalcitonin to Reduce Antibiotic Exposure during Acute Chest Syndrome in Adult Patients with Sickle-Cell Disease
Abstract
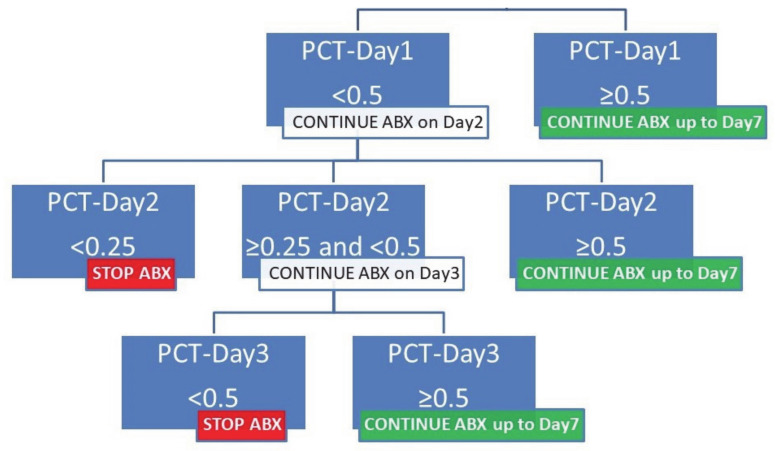
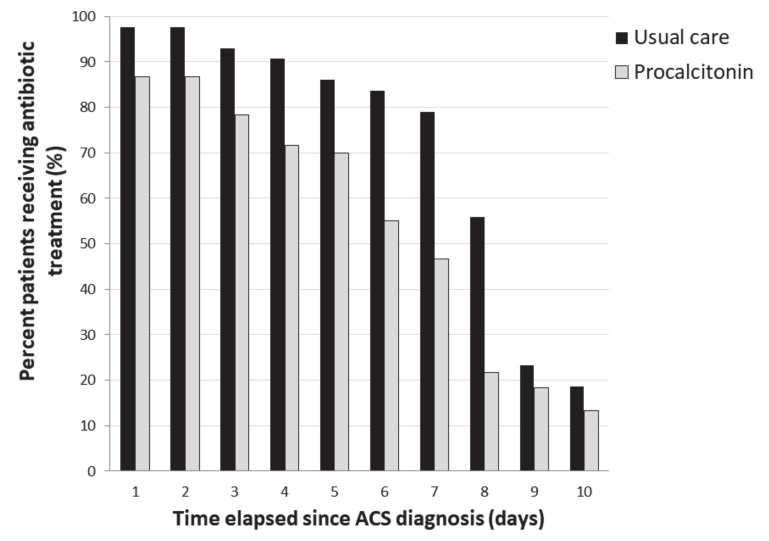
Acute chest syndrome (ACS) is a major complication of sickle-cell disease. Bacterial infection is one cause of ACS, so current guidelines recommend the routine use of antibiotics. We performed a prospective before-after study in medical wards and an intensive-care unit (ICU). During the control phase, clinicians were blinded to procalcitonin concentration results. We built an algorithm using the obtained measurements to hasten antibiotic cessation after three days of treatment if bacterial infection was not documented, and procalcitonin concentrations were all <0.5 μg/L. During the intervention period, the procalcitonin algorithm was suggested to physicians as a guide for antibiotic therapy. The primary endpoint was the number of days alive without antibiotics at Day 21. One-hundred patients were analyzed (103 ACS episodes, 60 in intervention phase). Possible or proven lung infection was diagnosed during 13% of all ACS episodes. The number of days alive without antibiotics at Day 21 was higher during the intervention phase: 15 [14-18] vs. 13 [13,14] days (p = 0.001). More patients had a short (≤3 days) antibiotic course during intervention phase: 31% vs 9% (p = 0.01). There was neither infection relapse nor pulmonary superinfection in the entire cohort. A procalcitonin-guided strategy to prescribe antibiotics in patients with ACS may reduce antibiotic exposure with no apparent adverse outcomes.
Keywords: acute chest syndrome; antibiotic; bacterial infection; procalcitonin; sickle-cell disease.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Vichinsky E.P., Neumayr L.D., Earles A.N., Williams R., Lennette E.T., Dean D., Nickerson B., Orringer E., McKie V., Bellevue R., et al. Causes and outcomes of the acute chest syndrome in sickle cell disease. National Acute Chest Syndrome Study Group. N. Engl. J. Med. 2000;342:1855–1865. doi: 10.1056/NEJM200006223422502. - DOI - PubMed
-
- Yawn B.P., Buchanan G.R., Afenyi-Annan A.N., Ballas S.K., Hassell K.L., James A.H., Jordan L., Lanzkron S.M., Lottenberg R., Savage W.J., et al. Management of sickle cell disease: Summary of the 2014 evidence-based report by expert panel members. JAMA. 2014;312:1033–1048. doi: 10.1001/jama.2014.10517. - DOI - PubMed
-
- Habibi A., Arlet J.-B., Stankovic K., Gellen-Dautremer J., Ribeil J.-A., Bartolucci P., Lionnet F. Centre de référence maladies rares «syndromes drépanocytaires majeurs» [French guidelines for the management of adult sickle cell disease: 2015 update] Rev Med. Interne. 2015;36:5S3–5S84. doi: 10.1016/S0248-8663(15)60002-9. - DOI - PubMed
LinkOut - more resources
Full Text Sources
