

Tailored immunosuppression after kidney transplantation - a single center real-life experience
- PMID: 33228545
- PMCID: PMC7686677
- DOI: 10.1186/s12882-020-02137-5
Tailored immunosuppression after kidney transplantation - a single center real-life experience
Abstract
Background: Kidney allograft survival continuously improved with introduction of novel immunosuppressants. However, also immunologically challenging transplants (blood group incompatibility and sensitized recipients) increase. Between 2006 and 2008, a new tailored immunosuppression scheme for kidney transplantation was implemented at the University Hospital in Zurich, together with an ABO-incompatible transplant program and systematic pre- and posttransplant anti-human leukocyte antigen (HLA) antibody screening by Luminex technology. This study retrospectively evaluated the results of this tailored immunosuppression approach with a particular focus on immunologically higher risk transplants.
Methods: A total of 204 consecutive kidney transplantations were analyzed, of whom 14 were ABO-incompatible and 35 recipients were donor-specific anti-HLA antibodies (DSA) positive, but complement-dependent cytotoxicity crossmatch (CDC-XM) negative. We analyzed patient and graft survival, acute rejection rates and infectious complications in ABO-compatible versus -incompatible and in DSA positive versus negative patients and compared those with a historical control group.
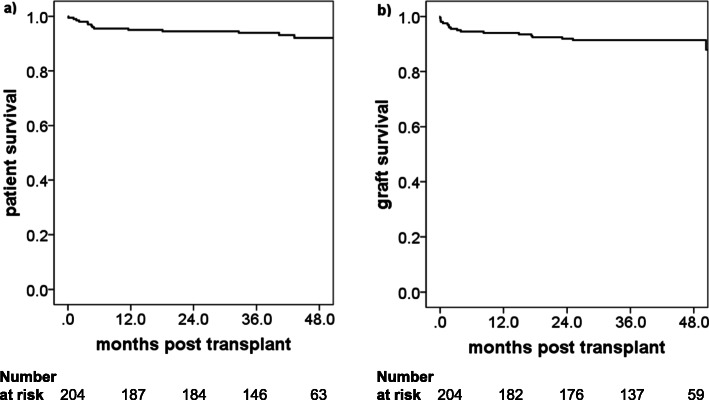
Results: Overall patient, death-censored allograft survival and non-death-censored allograft survival at 4 years were 92, 91 and 87%, respectively. We found that (1) there were no differences between ABO-compatible and -incompatible and between DSA positive and DSA negative patients concerning acute rejection rate and graft survival; (2) compared with the historical control group there was a significant decrease of acute rejection rates in sensitized patients who received an induction with thymoglobulin; (3) there was no increased rate of infection among the patients who received induction with thymoglobulin compared to no induction therapy.
Conclusions: We observed excellent overall mid-term patient and graft survival rates with our tailored immunosuppression approach. Induction with thymoglobulin was efficient and safe in keeping rejection rates low in DSA positive patients with a negative CDC-XM.
Keywords: ABO-incompatibility; Donor-specific antibodies; Induction therapy; Kidney transplantation; Rejection; Thymoglobulin.
Conflict of interest statement
The authors have no conflict of interest to declare with respect of this work.
Figures



References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
