

The predicted impact of tuberculosis preventive therapy: the importance of disease progression assumptions
- PMID: 33228580
- PMCID: PMC7684744
- DOI: 10.1186/s12879-020-05592-5
The predicted impact of tuberculosis preventive therapy: the importance of disease progression assumptions
Abstract
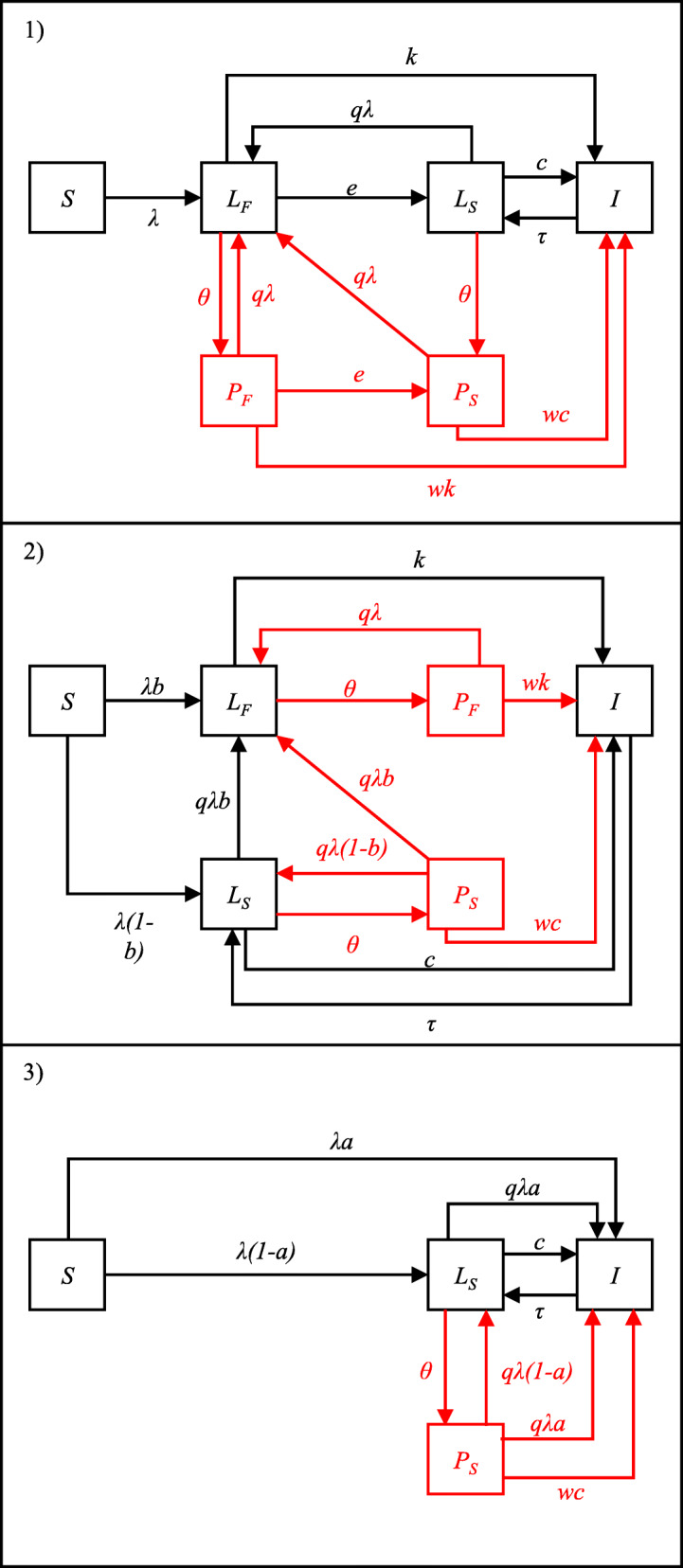
Background: Following infection with Mycobacterium tuberculosis (M.tb), individuals may rapidly develop tuberculosis (TB) disease or enter a "latent" infection state with a low risk of progression to disease. Mathematical models use a variety of structures and parameterisations to represent this process. The effect of these different assumptions on the predicted impact of TB interventions has not been assessed.
Methods: We explored how the assumptions made about progression from infection to disease affect the predicted impact of TB preventive therapy. We compared the predictions using three commonly used model structures, and parameters derived from two different data sources.
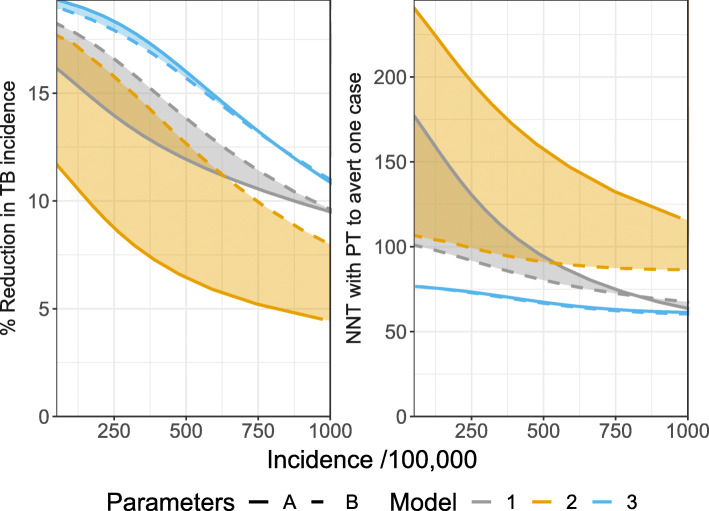
Results: The predicted impact of preventive therapy depended on both the model structure and parameterisation. At a baseline annual TB incidence of 500/100,000, there was a greater than 2.5-fold difference in the predicted reduction in incidence due to preventive therapy (ranging from 6 to 16%), and the number needed to treat to avert one TB case varied between 67 and 157. The relative importance of structure and parameters depended on baseline TB incidence and assumptions about the efficacy of preventive therapy, with the choice of structure becoming more important at higher incidence.
Conclusions: The assumptions use to represent progression to disease in models are likely to influence the predicted impact of preventive therapy and other TB interventions. Modelling estimates of TB preventive therapy should consider routinely incorporating structural uncertainty, particularly in higher burden settings. Not doing so may lead to inaccurate and over confident conclusions, and sub-optimal evidence for decision making.
Keywords: Modelling; Structure; Tuberculosis; Uncertainty.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Sutherland I. The ten-year incidence of clinical tuberculosis following "conversion" in 2550 individuals aged 14 to 19 years in TSRU Progress Report. The Hague: KNCV; 1968.
-
- Chiang C, Riley L. Exogenous reinfection in tuberculosis. Lancet Infect Dis. 2005;5(10):629–36. - PubMed
-
- Sanchez MA, Blower SM. Uncertainty and sensitivity analysis of the basic reproductive rate: Tuberculosis as an example. AJE. 1997;145(12):1127–37. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
