

Clinical outcome of biportal endoscopic revisional lumbar discectomy for recurrent lumbar disc herniation
- PMID: 33228753
- PMCID: PMC7685633
- DOI: 10.1186/s13018-020-02087-6
Clinical outcome of biportal endoscopic revisional lumbar discectomy for recurrent lumbar disc herniation
Abstract
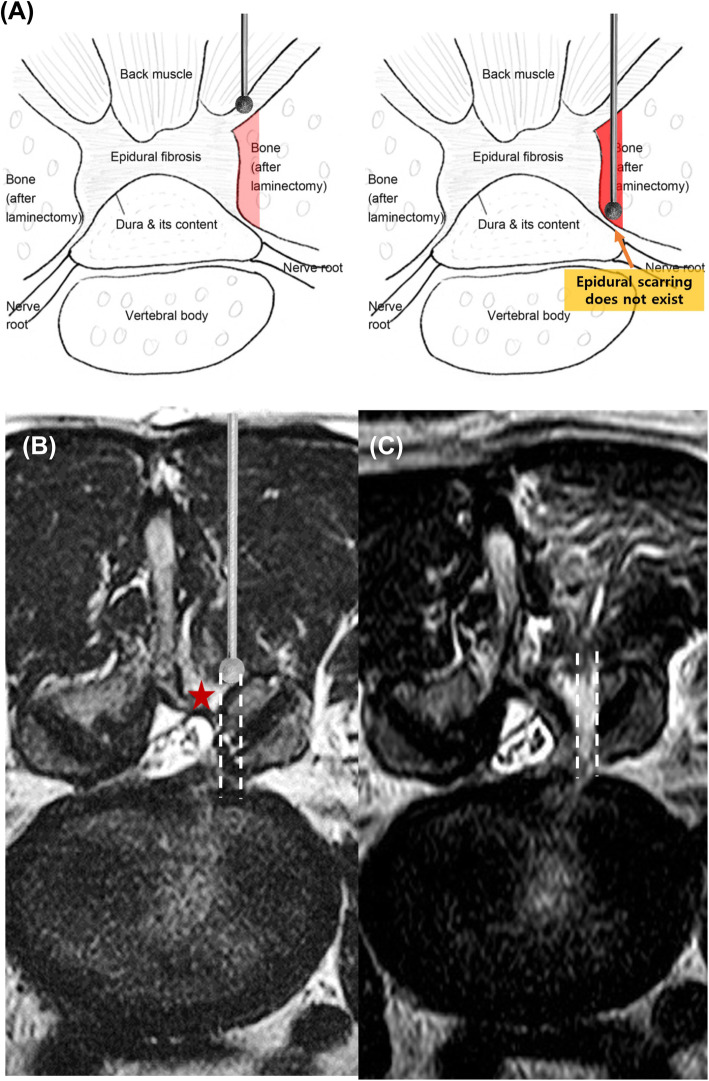
Background: Although literature provides evidence regarding the superiority of surgery over conservative treatment in patients with lumbar disc herniation, recurrent lumbar disc herniation (RLDH) was the indication for reoperation in 62% of the cases. The major problem with revisional lumbar discectomy (RLD) is that the epidural scar tissue is not clearly isolated from the boundaries of the dura matter and nerve roots; therefore, unintended durotomy and nerve root injury may occur. The biportal endoscopic (BE) technique is a newly emerging minimally invasive spine surgical modality. However, clinical evidence regarding BE-RLD remains limited. We aimed to compare the clinical outcomes after performing open microscopic (OM)-RLD and BE-RLD to evaluate the feasibility of BE-RLD.
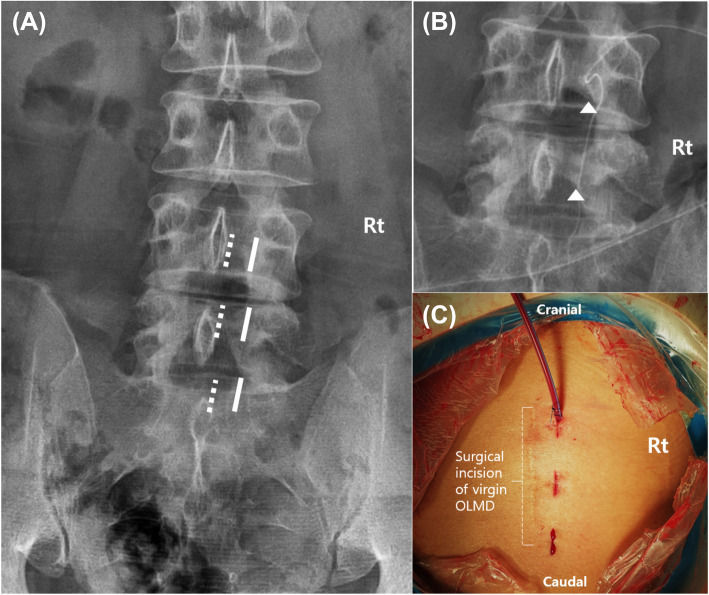
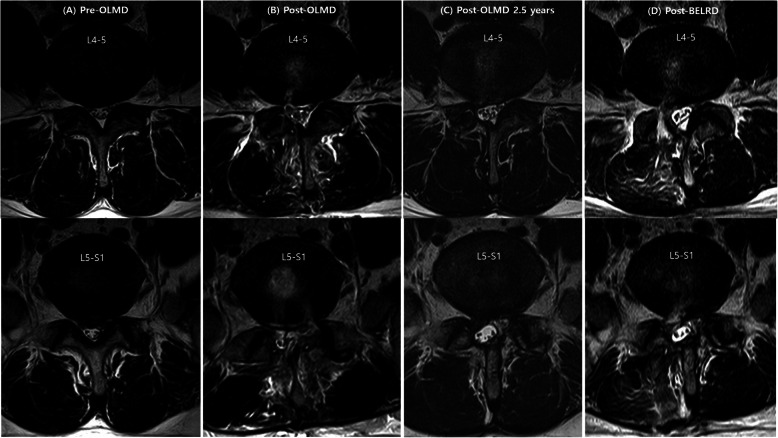
Methods: This retrospective study included 36 patients who were diagnosed with RLDH and underwent OM-RLD and BE-RLD. RLDH is defined as the presence of herniated disc material at the level previously operated upon in patients who have experienced a pain-free phase for more than 6 months. BE-RLD was performed as follows: two independent surgical ports were made inside the medial pedicular line of the target segment and on the intact upper and lower laminas. Peeling off the soft tissue from the vertebral lamina helps to easily identify the traversing nerve root and the recurrent disc material without dealing with the fibrotic scar tissue. Clinical outcomes were obtained using a visual analog scale (VAS) and the modified Macnab criteria before and at 2 days, 2 and 6 weeks, and 3, 6, and 12 months after surgery.
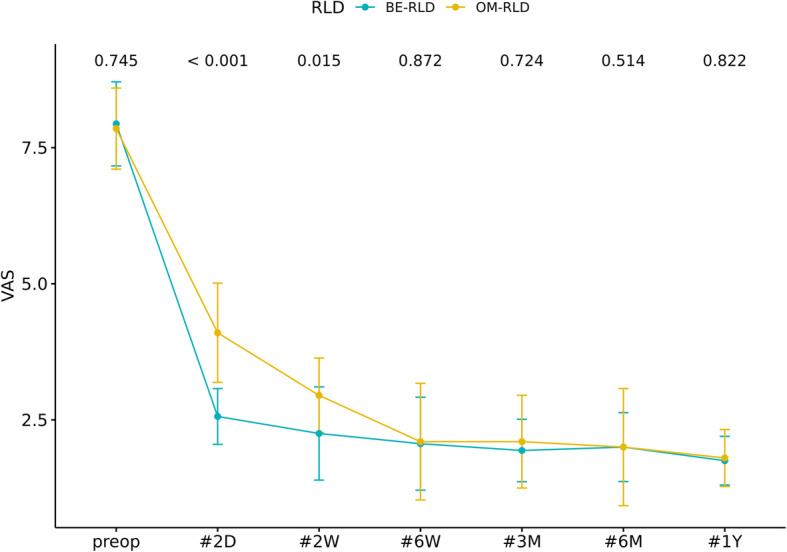
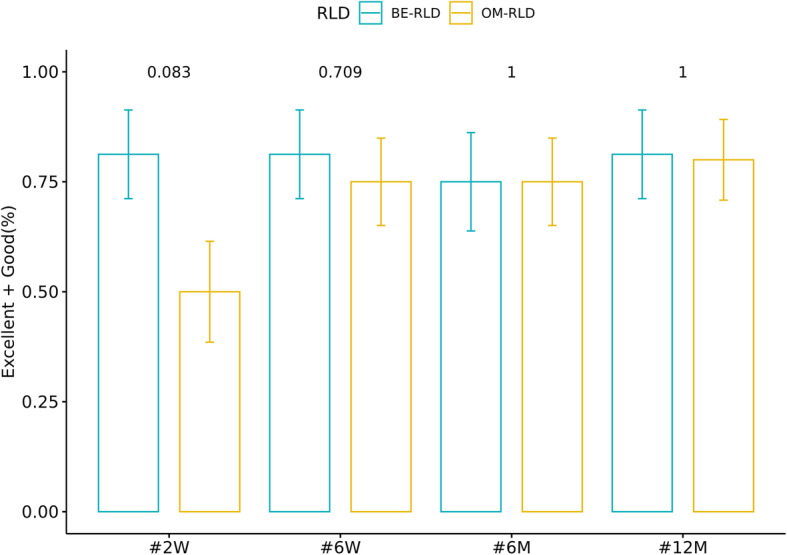
Results: The data of 20 and 16 patients who underwent OM-RLD and BE-RLD, respectively, were evaluated. The demographic and perioperative data were comparable between the groups. During the year following the surgery, in the BE-RLD group, the VAS scores at each point were significantly improved over the baseline and remained improved up to 2 weeks after surgery (p < 0.05); however, no statistical difference between the two groups was observed after 6 weeks of surgery (p > 0.05). According to the modified Macnab criteria on the follow-up, the excellent or good satisfaction rates reported at 2 weeks, 6 weeks, 6 months, and 12 months after surgery were 81.25%, 81.25%, 75%, and 81.25%, respectively, in the BE-RLD group, and 50%, 75%, 75%, and 80%, respectively, in the OM-RLD group.
Conclusion: BE-RLD yielded similar outcomes to OM-RLD, including pain improvement, functional improvement, and patient satisfaction, at 1 year after surgery. However, faster pain relief, earlier functional recovery, and better patient satisfaction were observed when applying BE-LRD.
Trial registration: Retrospectively registered.
Keywords: Biportal endoscopic; Lumbosacral radiculopathy; Open microscopic; Recurrent lumbar disc herniation; Revisional lumbar discectomy.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
