

Unusual case of upper gastrointestinal haemorrhage secondary to a ruptured gastroduodenal artery pseudoaneurysm: case presentation and literature review
- PMID: 33229478
- PMCID: PMC7684653
- DOI: 10.1136/bcr-2020-236463
Unusual case of upper gastrointestinal haemorrhage secondary to a ruptured gastroduodenal artery pseudoaneurysm: case presentation and literature review
Abstract
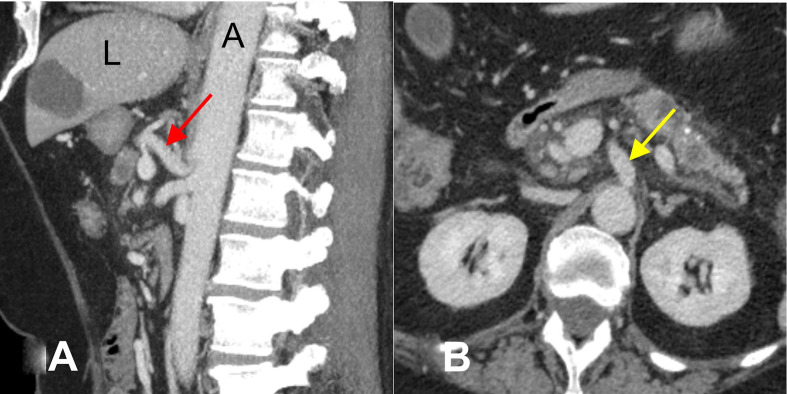
Pseudoaneurysm rupture of the gastroduodenal artery (GDA) is life-threatening and can present as an acute upper gastrointestinal haemorrhage. Here, we present a case of upper gastrointestinal haemorrhage arising from a ruptured GDA pseudoaneurysm. A 56-year-old woman presented acutely with haematemesis. She reported ongoing upper epigastric pain for a few weeks. Laboratory evaluation revealed severe microcytic hypochromic anaemia (haemoglobin, 69 g/L; normal, 120-140 g/L) and a mildly raised serum amylase level. Upper gastrointestinal endoscopy revealed dark blood collection between the rugae of the distal stomach. An abdominal CT scan detected a homogeneously enhancing rounded lesion arising from the GDA adjacent to the second part of the duodenum. The median arcuate ligament was causing stenosis of the coeliac axis origin. The diagnosis of haematemesis secondary to a ruptured GDA pseudoaneurysm was confirmed by mesenteric angiography, and aneurysmal embolisation was done. The haemoglobin level stabilised after aneurysmal embolisation.
Keywords: GI bleeding; interventional radiology; medical education; radiology.
© BMJ Publishing Group Limited 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures






Similar articles
-
Gastroduodenal Artery (GDA) Pseudoaneurysm as a Cause of Massive Upper Gastrointestinal (GI) Bleeding Years After Partial Gastrectomy.J Investig Med High Impact Case Rep. 2025 Jan-Dec;13:23247096251323076. doi: 10.1177/23247096251323076. Epub 2025 Mar 22. J Investig Med High Impact Case Rep. 2025. PMID: 40119668 Free PMC article.
-
Gastroduodenal artery pseudoaneurysm ruptured in the common bile duct.Acta Chir Belg. 2010 Jan-Feb;110(1):103-5. doi: 10.1080/00015458.2010.11680579. Acta Chir Belg. 2010. PMID: 20306924
-
Pseudoaneurysm of the gastroduodenal artery: an unusual cause for hyperamylasaemia.BMJ Case Rep. 2018 Apr 11;2018:bcr2017223882. doi: 10.1136/bcr-2017-223882. BMJ Case Rep. 2018. PMID: 29643139 Free PMC article.
-
Acute cholecystitis with massive upper gastrointestinal bleed: a case report and review of the literature.BMC Gastroenterol. 2007 Mar 26;7:12. doi: 10.1186/1471-230X-7-12. BMC Gastroenterol. 2007. PMID: 17386110 Free PMC article. Review.
-
Visceral artery pseudoaneurysms: two case reports and a review of the literature.J Med Case Rep. 2017 May 4;11(1):126. doi: 10.1186/s13256-017-1291-6. J Med Case Rep. 2017. PMID: 28472975 Free PMC article. Review.
Cited by
-
Refractory Duodenal Ulcer in a Patient With Median Arcuate Ligament Compression: A Treatment Challenge.ACG Case Rep J. 2024 Aug 5;11(8):e01407. doi: 10.14309/crj.0000000000001407. eCollection 2024 Aug. ACG Case Rep J. 2024. PMID: 39108613 Free PMC article.
-
Pseudoaneurysm of the Gastroduodenal Artery: A Rare Complication of Bile Duct Surgery.Cureus. 2024 Jan 30;16(1):e53209. doi: 10.7759/cureus.53209. eCollection 2024 Jan. Cureus. 2024. PMID: 38425630 Free PMC article.
-
Case report: Duodenal obstruction caused by gastroduodenal artery pseudoaneurysm with hematoma: an unusual case and literature review.Front Med (Lausanne). 2023 Jun 22;10:1198378. doi: 10.3389/fmed.2023.1198378. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37425331 Free PMC article.
-
Effective use of endoscopic ultrasound for diagnosing and differentiating a gastroduodenal artery aneurysm.Endoscopy. 2024 Dec;56(S 01):E1090-E1091. doi: 10.1055/a-2489-8203. Epub 2024 Dec 10. Endoscopy. 2024. PMID: 39657922 Free PMC article. No abstract available.
-
Gastroduodenal Artery Pseudoaneurysm Causing Upper Gastrointestinal Bleeding.Cureus. 2025 Jul 12;17(7):e87799. doi: 10.7759/cureus.87799. eCollection 2025 Jul. Cureus. 2025. PMID: 40799880 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical